

What is a fascia iliaca block (FIB)?
• A fascia iliaca block is an injection of local anaesthetic into the fascia iliaca compartment in the hip to provide pain relief to a patient awaiting hip fracture surgery.
• It blocks three specific nerves, the lateral cutaneous, femoral and obturator, providing broad pain relief.
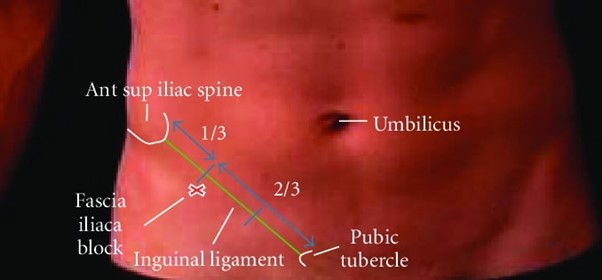
• The “landmark” technique of administering the FIB involves pinpointing the correct site for the injection by identifying two bony protuberances of the pelvis — the anterior superior iliac spine and the pubic tubercle. The injection is delivered below the inguinal ligament which runs between the two bone markers.
Older adults with hip fractures can often experience delays for surgery, which can leave them in severe pain while waiting in a ward for their operation.
The acute pain service nurses at Palmerston North Hospital saw an opportunity to improve pre-operative pain management for patients with a fractured hip, which led to their upskilling in the use of the fascia iliaca block.
This article describes the vision, aims and outcomes of this journey as implemented by the acute pain service team, which is made up of a nurse practitioner (NP) and three clinical nurse specialists (CNS), supported by anaesthetists. The acute pain service is a part of the local hip fracture working group.
Background
Pain relief in the form of local anaesthetic blocks injected in the hip was being given to patients with hip fractures in the Palmerston North emergency department (ED) by ED doctors, but often due to time pressure, patients were sent to the ward without a fascia iliaca block (FIB), which provides more comprehensive pain relief.
This, combined with delays in going to theatre, meant that some patients were experiencing severe pain while waiting for surgery. These patients were then more likely to receive regular opioid analgesics with unintended detrimental side effects.
It became clear the acute pain service could fulfil a role managing patients with a hip fracture who were admitted to the ward without receiving a FIB in ED or by ambulance staff, or those for whom surgery was delayed and therefore required a second FIB.
Discussions between the acute pain service and the lead pain/anaesthetic consultant led to a training programme for the acute pain service nurses to safely perform and administer FIB using the landmark procedure on patients in their ward awaiting surgery.
The “landmark” procedure for administering an FIB involves pinpointing the correct site for the injection by identifying two bony protuberances of the pelvis — the anterior superior iliac spine and the pubic tubercle. The injection is delivered below the inguinal ligament which runs between the two bone markers.
Hip fractures cause significant disability
Hip fractures cause significant disability for many older adults, with some of the worst outcomes for those aged 65 years or older, affecting more women than men.1, 11 Having a hip fracture in later life can lead to long recovery periods, decreased quality of life, higher mortality rates and increased likelihood of entry into aged residential care, compared to those without a hip fracture.1, 2, 3
Pain is a significant feature of a hip fracture, causing discomfort and distress to the person and their family/whānau.4 Untreated pain can have adverse effects on physical and psychological wellbeing such as catabolism (where stress hormones break down body tissues), increased activity in the sympathetic nervous system (“fight or flight” physiological reactions), suppression of the immune system, increased anxiety, loss of sleep and feelings of helplessness.5, 6
Pre-operative pain management
Surgery is recommended for most patients with a hip fracture, with the goal of alleviating pain and improving function. Surgical intervention itself is usually the most effective form of analgesia.4 However hip-fracture patients will often have an extended waiting time before surgery is available. Hence, effective pre-operative pain management for patients with hip fracture is a priority.
Hip fracture is more common in people with dementia,10, 11 and people with fractured hips are at high risk of delirium (some studies saying the risk to be as high as 60 per cent12), particularly if they are administered opioid analgesia. A 2008 study also noted dementia patients “were unable to request analgesia and often were not prescribed or given adequate pain relief, resulting in unnecessary suffering”.10
The ability for acute pain service nurses to administer FIB blocks represents new practice that previously was undertaken by medical staff.
Analgesia can be administered systemically or locally. Systemic analgesic options include paracetamol, which should be offered every six hours unless contraindicated, and opioid analgesics.4
Opioids should only be used for the management of severe acute pain at the lowest effective dose for the shortest possible duration.7 While being an effective analgesic for severe acute pain, opioids cause a considerable number of harms, such as ventilatory impairment, constipation and confusion.8, 9
Using local anaesthetic options reduces complications such as respiratory depression, sedation, and delirium. Use of local anaesthetic blocks is recommended, to reduce the amount of opioid a patient is given or if the opioid is ineffective in managing the pain. However a local anaesthetic nerve block should not be used as a substitute for early surgery.4
The FIB block is a straightforward and proven method for managing acute pain following hip fracture.
The repeating of a fascia iliaca compartment block seemed a commonsense approach to relieve pain when surgery was delayed. The block is simple, fast acting, reliable and considered safe.10 Three nerves — the lateral cutaneous, femoral and obturator — pass through the fascia iliaca compartment, and all are affected by the block.10
The FIB block has been tested in several settings and is a straightforward and proven method for managing acute pain following hip fracture.
Acute pain service nurses trained
The acute pain service nurses at Palmerston North have now been endorsed to perform the FIB using the landmark procedure, after undergoing training with a specialist consultant anaesthetist.
All patients that present with a hip fracture are now referred to the acute pain service, which then decides the most appropriate pain management plan before surgery. In some cases, this involves administering a FIB preoperatively or if surgery is delayed.
In the past, this would mean contacting the duty anaesthetist and organising the patient to be brought to theatre when a space was available for the anaesthetist to place a femoral nerve block under ultrasound guidance. At this hospital, the ability of acute pain service nurses to administer FIB blocks represents new practice that was previously undertaken by medical staff.
New practice audited
To assess the effectiveness of this new practice, an audit was undertaken of patients with a hip fracture who received a FIB for pain relief carried out by a member of the acute pain service over a period of 13 months.
Twenty-five patients were included in the audit, seven with dementia. One patient received two blocks from the acute pain service due to delays in surgery, which meant 26 blocks were audited. The audited patients comprised 18 females and seven males with an age range of 54-99 years.
The audit looked at five different measures: pain scale pre- and post-block, opioid use pre- and post-block and patient satisfaction with block.
The acute pain service team used the landmark procedure to deliver their FIB (as shown below in figure 1).13 Patients weighing less than 50kg received 30ml 0.2% Ropivacaine, and for those weighing more than 50kg, 40ml 0.2% Ropivacaine.
These parameters for dosing mean the volume is sufficient for analgesic effect, yet well within the margin for toxicity. When a second dose was required, there was a stand down of six hours. There were no recorded complications from these procedures.
Pain scores were assessed using a visual analogue scale (VAS) except when this was inappropriate, such as for those patients with dementia. In this case the Abbey Pain Scale was used.
Pain scores on presentation for all patients at rest was between 4/10 and 10/10 with an average of 6.9/10. The same was true on movement, with pain rated between 4/10 and 10/10 with an average of 7.3. In comparison, the post-block pain scores were low — these scores were taken on movement at 15 minutes, two hours, eight hours, and 24 hours. The average rating was 2/10 at 15 minutes, 1.3/10 at two hours, 2.2/10 at eight hours, and 3.5/10 at 24 hours.
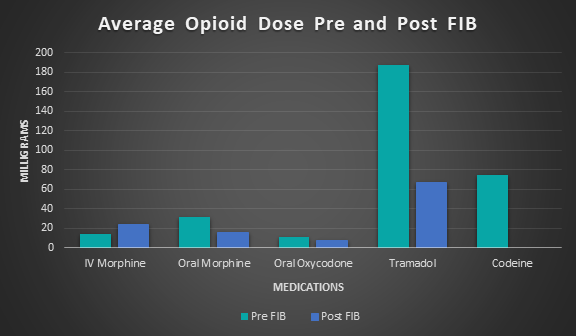
The audit compared opioid use before and after the block, which showed significant differences. The opioids used to control pain in the patients in this audit were limited to oral and intravenous (IV) morphine, oral oxycodone, tramadol and codeine.
Overall, post-FIB there was a reduction in the amount of opioids administered (see figure 2). However, due to three of the blocks being ineffective, patients given IV morphine increased by 66 per cent, from 14mg pre-FIB to 24mg post FIB. The remaining audited patients clearly showed decreased average opioid dosage post-FIB, where oral morphine was reduced by 48 per cent, oxycodone reduced by 22 per cent, tramadol by 58 per cent and codeine by 100 per cent.
Patients were asked to rate the effectiveness of the FIB in providing pain relief 24 hours after the block, using the Likert scale, with 1 being very poor to 5 which was excellent. The range was between 2-5 with the average being 4.2 which correlates with a good-excellent rating (see figure 3).
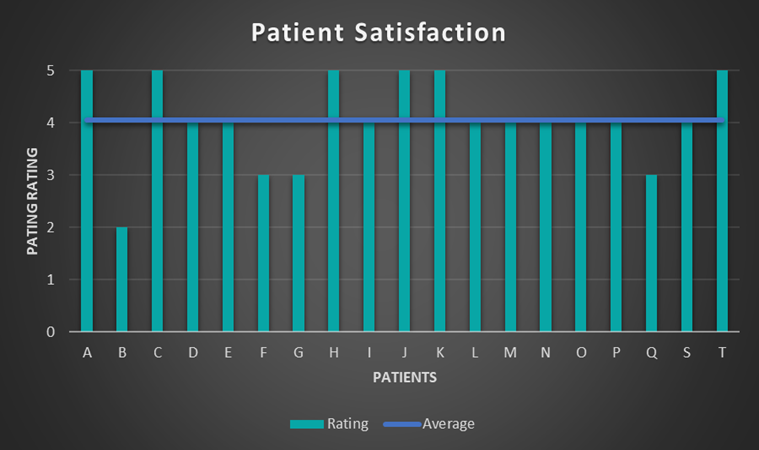
Results demonstrated that a FIB is highly effective in the management of the pain associated with hip fracture. Interpreting the data, it is clear three of our patients did not receive significant benefit from their FIB and were the only patients to receive IV opioids after the block was given. In each of these cases, the patient still rated their satisfaction with their pain management as “good”.
There were seven patients with a diagnosis of dementia who were part of our audit, and we used the Abbey Pain Scale to assess their pain. This is an internationally validated tool to help staff assess pain in patients with dementia and/or delirium, who cannot express how they feel. It uses measures including the way the patient vocalises, their facial expressions and body language, and behavioural and physical changes.
For all seven, the block was effective. The average pain score at 15 minutes and two hours being 0/10, the average at eight hours 1.3/10 and at 24 hours 1.9/10. This represents an excellent outcome for such an at-risk group.
The effective management of pain without the use of systemic opioids in the population who suffer a hip fracture has led to a reduction of the incidence of opioid-induced confusion and other additional complications. This audit has shown the inclusion of patients with a diagnosis of dementia has led to positive outcomes, particularly as this group has difficulty articulating their needs and their pain to nursing staff.
This audit highlighted an important issue of our time and the complexities associated with delays in surgery. The Australian and New Zealand Guideline for Hip Fracture Care4 is a programme that, in ideal circumstances, delivers safe and timely care for patients suffering from a hip fracture. This audit indicates that the pressure on EDs and operating theatre space means hospitals are currently unable to fulfill the guideline for hip fracture care in its entirety.
The audit showed that RNs and NPs with appropriate training can deliver a FIB in a safe and timely fashion, providing a solution to fulfilling the criteria for hip fracture care.
Issues for extending RN practice
This extension of RN practice highlighted some issues to consider. These are:
- RNs need training and assessment to undertake the FIB landmark procedure.
- An FIB for hip fracture care involves prescribing medication which can be an obstacle to delivering the procedure, particularly after hours. Although three CNSs on the acute pain service team have prescribing rights, regulations at the time of writing this article prevented RN prescribers from prescribing local anaesthetics required for FIBs. This limits their ability to independently deliver the procedure. A way of improving this service would be to implement standing orders for the acute pain service nurses. (NB: In December 2025, the Nursing Council issued an updated drugs list which now authorises designated RN prescribers to prescribe Ropivacaine, a local anaesthetic used for FIBs.)
- The delivery of a FIB service increases the acute and unplanned workload for the RN/NP in the acute pain service. This requires a commitment to ensure that the current FTE allocation meets both patient and service needs.
Hip fractures are painful, and pain, left untreated, can result in a host of complications that may delay the patient’s surgery and complicate their hospital stay. Medical doctors have historically been responsible for inserting FIBs but several studies have shown specialist-trained nurses are capable of inserting FIBs successfully and safely.
Overall, FIB given preoperatively by trained acute pain service staff is safe, while reducing opioid consumption and improving patient satisfaction post a hip fracture.
The initiative to administer FIBs was primarily undertaken to improve outcomes for patients with a hip fracture; however there were significant positive unintended outcomes. Firstly, being involved in this initiative increased the autonomy and extended the practice of the acute pain service nurses. Secondly, it empowered them to advance and lead nursing practice in the field of pain management.
Overall, FIB given preoperatively by trained acute pain service staff is safe, while reducing opioid consumption and improving patient satisfaction post a hip fracture.
This study has highlighted issues that may arise in services without the ability to prescribe medicines or those that have restricted lists to prescribe from. Further work is needed to ensure that the process is timely and safe.
While patients with dementia were included in this study’s cohort, a larger study reviewing the pain issues of hip-fracture patients with delirium and dementia could be considered.

James Camacaylan, RN, MN, is a clinical nurse specialist; Lisa Clince, RN, MN, is a clinical nurse specialist; Erica Gleeson, NP, is a nurse practitioner; and Grant McCullough, RN, MN, is a clinical nurse specialist. Together they make up the acute pain service at Palmerston North Hospital. This service provides expert pain management, supporting patients through their recovery, and providing education to clinical teams under the guidance of the anaesthetic department.
- This article was reviewed by Paddy Holbrook, RN, NP, an emergency department nurse practitioner and senior clinical lecturer in the nursing department, University of Otago, Christchurch.
References
- Keller, J. M., Sciadini, M. F., Sinclair, E., & O’Toole, R. V. (2012). Geriatric trauma: demographics, injuries, and mortality. Journal of Orthopaedic Trauma, 26(9), e161-e165.
- Ariza-Vega, P., Jiménez-Moleón, J. J., & Kristensen, M. T. (2014). Change of residence and functional status within three months and one year following hip fracture. Disability and Rehabilitation, 36(8), 685-690.
- Marks, R. (2010). Hip fracture epidemiological trends, outcomes, and risk factors, 1970–2009. International Journal of General Medicine, 3, 1-17.
- Chehade, M., & Taylor, A. (2014). Australian and New Zealand guideline for hip fracture care — improving outcomes in hip fracture management of adults. Australian and New Zealand Hip Fracture Registry (ANZHFR) Steering Group 2014.
- Hanks-Bell, M., Halvey, K., & Paice, J. (2004). Pain assessment and management in aging. Online Journal of Issues in Nursing, 9(3).
- Schug, S. A., Palmer, G. M., Scott, D. A., Alcock, M., Halliwell, R., & Mott, J. (Eds.). (2020). Acute pain management: Scientific evidence. Australian and New Zealand College of Anaesthetists.
- Dowell, D., Ragan, K. R., Jones, C. M., Baldwin, G. T., & Chou, R. (2022). CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recommendations and Reports, 71(3), 1-95.
- Health Quality & Safety Commission. (2022). Safe use of opioids.
- Davies, P. S. (2017). Opioids for pain management in older adults: Strategies for safe prescribing. The Nurse Practitioner, 42(2), 20-26.
- Macaulay, W., Pagnotto, M. R., Iorio, R., Mont, M. A., & Saleh, K. J. (2006). Displaced femoral neck fractures in the elderly: hemiarthroplasty versus total hip arthroplasty. Journal of the American Academy of Orthopaedic Surgeons, 14(5), 287-293.
- Rawal, N. (Ed.). (1998). Management of acute and chronic pain. BMJ Books.
- Smith, T. O., Gilbert, A. W., Sreekanta, A., Sahota, O., Griffin, X. L., Cross, J. L., Fox, C., & Lamb, S. E. (2020). Enhanced rehabilitation and care models for adults with dementia following hip fracture surgery. Cochrane Database of Systematic Reviews, (2).
- Singh, Shiv & Gulyam Kuruba, S M. (2011). Landmarks for fascia iliaca compartment block [Image]. Research Gate.