
About the authors:Tarryn Jack, RN designated prescriber, PGDip Nsg, MN candidate, is a nurse prescriber at Tokoroa Family Health, South Waikato. Patricia McClunie-Trust, RN, PhD, is a principal lecturer in the Centre for Health and Social Practice, Waikato Institute of Technology, Hamilton. Her correspondence address is: [email protected] Author contributions: This article was accepted for publication in October 2025. |
ABSTRACTBackground: This meta-synthesis explores the lived experiences of individuals as they navigate their journey with gout. Nurses must recognise gout as a highly treatable condition, enabling them to deliver high-quality, relevant care to those affected. Objective: To explore the lived experiences of people with gout. Methods: A qualitative meta-synthesis was undertaken using meta-ethnography. Electronic databases searched included CINAHL Plus, PubMed and Medline. Qualitative studies published in English that reported rich descriptions of the lived experiences of people with gout were sought for inclusion. No date limiters were applied. Findings:Twenty primary research studies were selected for inclusion in this review. The overarching theme that emerged from the synthesis was the ripple effect from gout flares impacting a person’s entire life. Three subthemes and storylines were identified as Disrupted lives (Pain is disruptive), Misconceptions about gout (Misunderstanding and missed management), and Finding a sense of agency (Negotiating how to live with gout). Conclusion: People living with gout are confronted with challenges in the physical, mental, emotional and social aspects of everyday life. They are sometimes reluctant to seek treatment because of the assumption that it is self-inflicted and therefore should be silently endured. Nurses need to understand the lived experience of gout and the opportunities for providing optimal support, enabling individuals to manage their condition more effectively and increase their self-agency over their bodies, thereby reducing the impact that gout has on overall well-being. |
||
KEYWORDSgout, chronic disease, lived experience, stigma, pain, sense of agency |
|||


Introduction
THIS META-SYNTHESIS explores the lived experiences of individuals with gout as a chronic condition. Gout is the most prevalent and uniquely curable form of inflammatory arthritis worldwide (Doherty et al., 2012; Kuo et al., 2015). Although it is treatable, suboptimal treatment is widespread globally. Gout is notorious for acute, sporadic and debilitating episodes known as gout flares, resulting in severe pain and causing progressive disfigurement (Sivera et al., 2022). This pain can limit physical activity, leading to increased time off work, which affects earning capacity, reduces socialisation and affects mental health (Smith et al., 2011). The review question was framed as: What are the lived experiences of people with gout?
Background
Nurses need insight into the prevalence and lived experience of gout to provide good health care (Dehlin et al., 2020). The prevalence of gout worldwide ranges from 1 percent to 10 percent, depending on population demographics (Galassi et al., 2024). A greater prevalence is found in men and older populations, as well as in certain ethnic groups, suggesting a genetic predisposition (Galassi et al., 2024; Kuo et al., 2015). Oceanic countries, particularly those with significant populations of Taiwanese, Aboriginal, Pacific and Māori descent have the highest prevalence of gout. Along with ethnicity, other demographic factors also affect gout prevalence, including age and gender (Dehlin et al., 2020; Sivera et al., 2022). For instance, the prevalence of gout in New Zealand is among the highest internationally, affecting approximately 6 percent of the total population aged over 20 years (Dalbeth et al., 2018; BPACnz, 2021). The prevalence of gout among Māori is double that of European and other ethnicities, and the incidence of gout in Pacific peoples is triple that of European and other ethnicities (Gout, 2019).
People who experience the intial stages of gout are often unaware of the potential for it to develop into a chronic, disabling disease, which can affect their quality of life and become permanently disabling (Wertheimer et al., 2013). People living with chronic disease have complex needs, requiring a range of health-care services, which necessitate empowering the individual to self-manage their disease. Understanding the lived experience of people with chronic diseases such as gout empowers and motivates nurses to engage in patient-centred health-care management strategies. (Nolte, 2008).
As a chronic disease, gout progresses through four stages, starting with asymptomatic hyperuricemia and progressing to chronic pain and loss of function (Ragab et al., 2017). In the first stage, signalled by high levels of uric acid in the body, people have no symptoms (Afzal et al., 2025). In the second stage, the uric acid starts to form urate crystals which often collect in the joints, causing sudden, severe pain, swelling and heat, also known as a gout attack, or flare. While symptoms usually improve within two weeks with the use of anti-inflammatory medication or steroids, over time these flares may increase in frequency, severity and duration (Dalbeth et al., 2016; Smith & Karakashian, 2018; Wertheimer et al., 2013). During the third stage, people are mostly asymptomatic, and the condition appears to be resolved. However, the deposit of crystals from persistent hyperuricemia continues to build (Afzal et al., 2025). This stage is also referred to as inter-critical gout (Smith & Karakashian, 2018). The fourth stage is chronic tophaceous gout, which develops approximately 10 years from the first presentation, where earlier stages have been insufficiently treated (Afzal et al., 2025). This stage can destroy bones and joints, causing severe deformity and probable renal impairment (Smith & Karakashian, 2018).
The fact that gout is a chronic disease requires clear communication with patients to prevent misinterpretation that may hinder treatment (Talaat et al., 2021). Implementing a treatment plan formulated between the individual and the nurse involves educating individuals about how to monitor and manage symptoms by addressing underlying causes, and recommending both pharmacological and non-pharmacological treatments (Benn et al., 2018). Supporting people in managing the greater impact of gout involves educating them about a health-promoting lifestyle and making informed nutritional choices (Regan-Smith et al., 2022; Rimler et al., 2016). Clinical guidelines recommend long-term management with urate-lowering drug therapy, such as allopurinol, probenecid and febuxostat (Gill et al., 2020) to control gout. Initiating urate-lowering therapy using a dose-escalation strategy, combined with prophylactic low-dose anti-inflammatory therapies or colchicine, can reduce gout flares and is effective in achieving treatment targets (Dalbeth et al., 2019).
Education includes highlighting to the person with gout the likelihood that they are genetically predisposed to the condition to remove any perception that it is self-inflicted (Benn et al., 2018). Health practitioners must be cautious about enforcing unrealistic lifestyle and dietary modifications that may evoke feelings of self-blame (Pillinger & Mandell, 2020). There are effective and readily accessible treatments for gout. However, the disease burden of gout is increasing worldwide and is associated with significant morbidity (Meyappan et al., 2021).
Methods
Study design
The design of this study is qualitative meta-synthesis, informed by meta-ethnography. Meta-ethnography is one of the most developed methods for synthesising qualitative research studies on a particular topic (Hannes & Lockwood, 2012). It is an inductive approach that seeks to interpret multiple studies by integrating their findings (Sattar et al., 2021) to develop broader analytical insights, enabling a deeper understanding of a phenomenon. Meta-ethnography is particularly appropriate for developing conceptual models and theories, and can be used in health care to generate evidence and inform policy. France et al. (2019) propose that meta-ethnography can offer new insights into how patients perceive their health conditions, affect their adherence to treatment and enhance understanding of the effectiveness of interventions. There are seven phases in conducting a meta-synthesis using meta-ethnography (France et al., p. 2), as shown in Table 1.
Table 1. The seven phases in meta-ethnography
| Phase 1 | Identifying a phenomenon of interest that qualitative research might inform |
| Phase 2 | A systematic review of the literature |
| Phase 3 | Reading the studies |
| Phase 4 | Determining how the studies are related |
| Phase 5 | Translating the studies into one another |
| Phase 6 | Synthesising translations |
| Phase 7 | Expressing the synthesis |
Identifying a phenomenon
The phenomenon of interest was identified as the lived experience of gout, and the review question was framed using the PICo (Population, Phenomenon of Interest, Context) framework. The population consisted of adults, the phenomenon of interest was their lived experiences, and the context was gout.
Systematic review of the literature
A systematic search for peer-reviewed published qualitative studies on people’s experiences of living with gout was implemented with the assistance of an expert librarian. Electronic databases searched included CINAHL Plus, PubMed, MEDLINE, ScienceDirect, DOAJ, CORE, OVID and Cochrane, without date limiters, up to the final search date. Table 2 summarises the PICo structure used to frame the search for primary qualitative studies in response to the review question. The CINAHL search string is outlined in Table 3, and was adapted for use in the other database searches. The search strings table is set out in Supplementary File 1.
The electronic database references were exported and duplicates removed using citation management software (Zotero) before being imported into Covidence Systematic Review Software (Veritas Health Innovation, 2023) for screening. A hand search of the reference lists of the included studies was also undertaken to identify any additional articles that were not found through database searches.
Table 2: PICo table
| Key words | Synonyms | |
|---|---|---|
| P — Population | Adults | Adults |
| I — Phenomenon of interest | Lived experience | Experience, perceptions, thoughts, feelings, opinions, attitudes, beliefs or emotions |
| Co — Context | Gout | Gout, hyperuricemia |
Table 3: Search terms
Qualitative studies: The lived experience of gout
| Concepts | Additional key words | |
|---|---|---|
| Population | Adults | Adult* OR age* OR geriatric OR “old person” OR “elderly person” OR “middle age” OR senior OR “young adult” |
| I — Phenomenon of interest | Lived experience | Experience OR “lived experience” OR “patient experience” OR “personal experience” OR perception* OR thought* OR feeling* OR opinion* OR belief* OR attitude OR “attitude* to illness” OR emotion* |
| Context | Gout | Gout OR “gouty arthritis” OR hyperuricemia |
Study selection
Two reviewers, PM and TJ, undertook a two-stage blind screening process in Covidence. The reviewers independently screened title and abstract records, followed by full-text screening of records that potentially met the inclusion criteria. Conflicts in screening were resolved through consensus by the two reviewers.
Critical appraisal
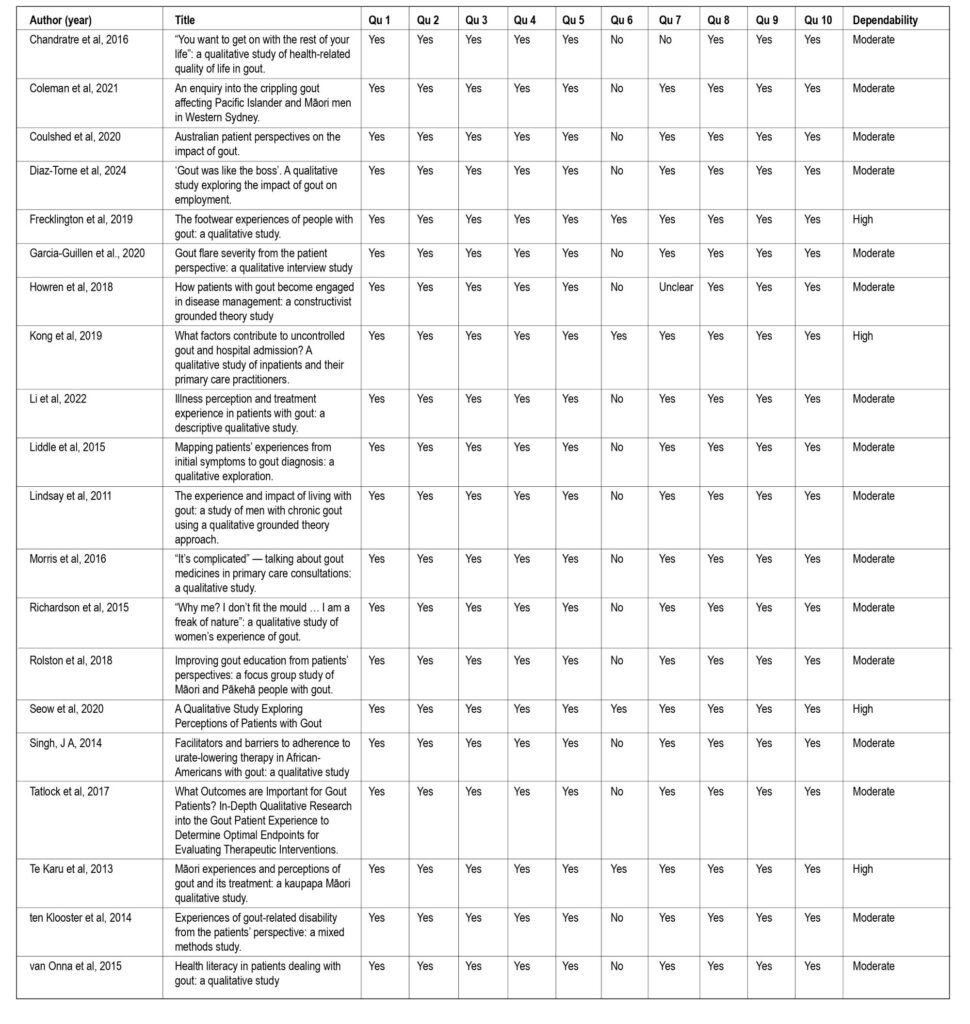
The included studies were critically appraised in duplicate (TJ & PM) using the JBI 10-item critical appraisal checklist for qualitative research studies (Porritt et al., 2024). A quality appraisal was undertaken to assess and report the methodological quality, including ethical review (Munn et al., 2018), and the results were tabulated and reported. All subsequent studies then proceeded to data extraction, tabulation and narrative summary. The critical appraisal table is included as Supplementary File 2.
Data extraction
Two reviewers (TJ & PM) independently extracted data into the predetermined fields of the data extraction framework in Covidence. The extraction fields included publication details, study design and objectives.
Data synthesis
Phase 3 marks the beginning of the synthesis (Sattar et al., 2021), during which researchers become familiar with key concepts and metaphors in each study by repeatedly reading the studies (Sattar et al., 2021). Phase 4 involves determining how the studies are related to “put them together” (Noblit & Hare, 1999, p.111). This phase involves determining how the different studies relate to one another (France et al., 2019) and formulating themes, concepts and metaphors to compare and contrast them (Atkins et al., 2008). Phase 5 involves translating the studies into one another (Noblit & Hare, 1999), which entails a meticulous comparison of the meanings of concepts and metaphors across different studies to determine the range of concepts. The key to translation is interpreting meaning (France et al., 2019). Reciprocal translation involves directly comparing and combining studies to gain a deeper understanding. Refutational translation occurs when the studies oppose one another. Phase 6 is the second-level synthesis, where translations from the previous phase are further developed by comparing them to identify similar concepts and form interpretations that extend beyond the findings from individual studies (France et al., 2019). The findings (Phase 7) are set out in the following section.
Results
Search strategy
The electronic database search produced 365 studies; 43 studies proceeded to full-text review, and 20 studies met the inclusion criteria. The search, screening and selection process is set out in Figure 1.
![]()
Characteristics of the included studies
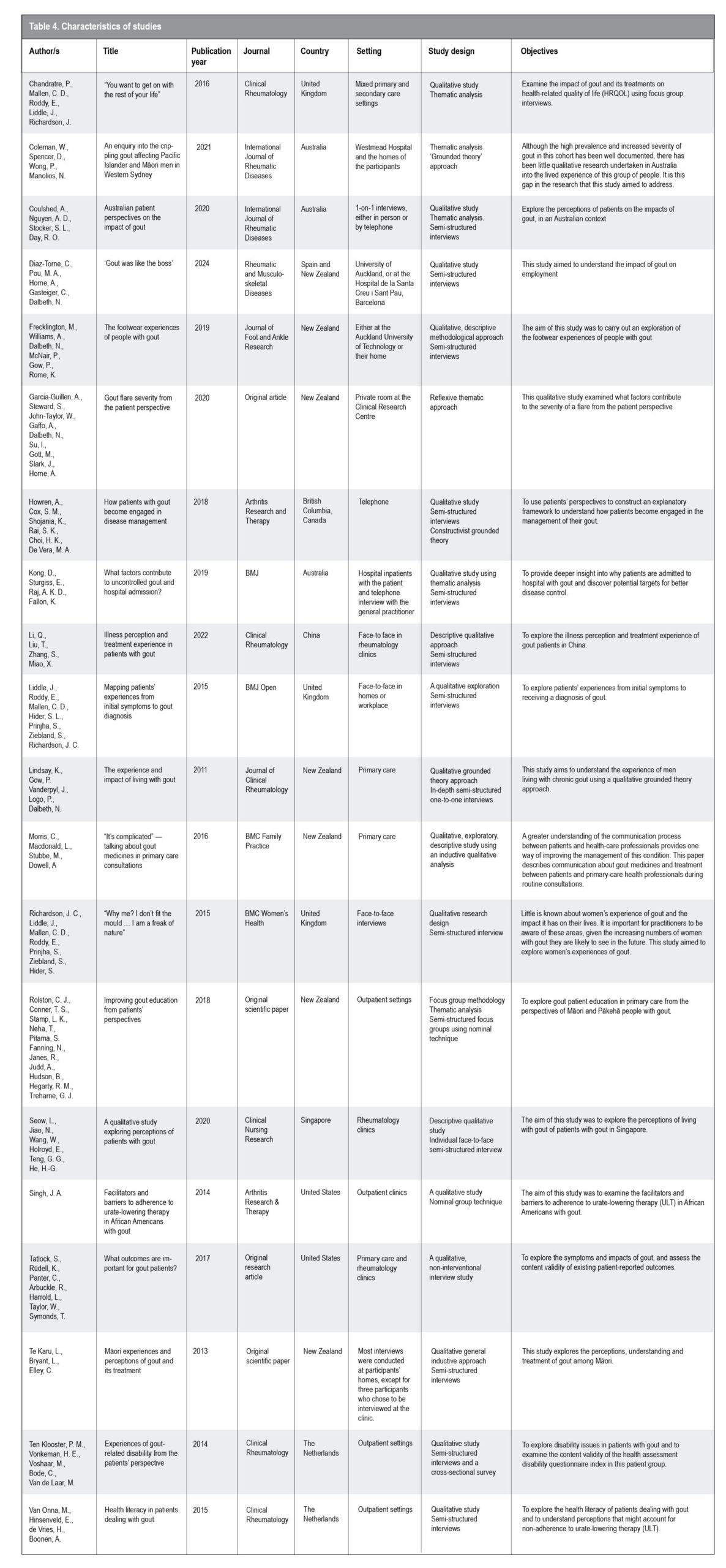
Twenty studies met the inclusion criteria for this meta-synthesis. All studies were published in English between 2011 and 2024. The studies were all primary studies, with two being original research and 18 published in journals. Studies originated from the United Kingdom, Australia, Spain, New Zealand, British Columbia, Canada, China, Singapore, the United States and the Netherlands. Seven of these studies were from New Zealand. Interviews were conducted in various settings, including primary and secondary care, people’s homes and workplaces. Most interviews were face-to-face, while some were conducted over the phone. The study designs were all qualitative; most studies were descriptive and explorative, two used a grounded theory approach, and one used a mixed-method approach. The characteristics of the included studies are summarised in Table 4.
Narrative presentation of findings
The overarching theme developed from the analysis was “The ripple effect from gout flares impacting on a person’s entire quality of life.” Three subthemes identified from the synthesis include: 1. Disrupted lives, 2. Misconceptions about gout, and 3. Finding a sense of agency. Figure 2 illustrates the ripple effect from gout flares.
Theme 1: Disrupted lives
Narrative storyline — Pain is disruptive
Severe pain from gout flares has a disruptive effect that leads to a sense of helplessness, due to loss of control. The ripple effect from severe pain caused by repeated gout attacks is multifaceted, negatively affecting the person’s quality of life. Participants in the studies described the all-consuming nature of severe gout in terms of its impact on perceived quality of life (Coleman et al., 2021). “The worst thing ever, man, gout. It’s just taken over my life, I can’t do anything” (Participant not identified, Coleman et al., 2021, p. 1398). Participants could recount their first experience of gout pain with vivid descriptions of the worst pain ever experienced, comparable with birth pains and heart attacks. Pain significantly affected their physical lives (Garcia-Guillen et al., 2020; Te Karu et al., 2013). “It just feels like the area is inflamed…cooking. I mean it is hot, a real hot sensation…it feels like the flesh is trying to rip your outside…like it is going to burst…” (P7, Lindsay et al., 2011, p. 2).
The severity of pain was dependent on the stage of gout, varying from a mild warning twinge settled by treatment to a severe debilitating flare that led to days bed-bound (Te Karu et al., 2013). “I just couldn’t move. The pain was that bad, you just wanted to cut your foot off. You can’t touch it, you can’t walk. You lose your appetite. You can’t work. It makes you miserable” (P9, Te Karu et al., 2013, p. 217). The impact of pain from chronic gout is evident in every step of daily life, having a disruptive effect on activities such as walking, preparing food and self-care (Coleman et al., 2021; Garcia-Guillen et al., 2020).
Participants with mild flares did not report the same degree of disruption to their lives. “It [gout] doesn’t [affect my life], it’s a bit uncomfortable for the first day, but you know it doesn’t stop me from doing anything” (P13, Coulshed et al., 2020, p.1376). However, other participants reported problems with activities associated with daily living, which negatively affected their sense of self-worth (Coulshed et al., 2020; Garcia-Guillen et al., 2020). “When it’s at its worst…it was difficult to even just get out of bed… shower, toilet. All those daily things, it was… very difficult.” (P19, Garcia-Guillen et al., 2020, p. 18). Sleep was a luxury for some participants due to unrelieved pain during an acute attack (Garcia-Guillen et al., 2020). “When it hits hard, you can’t even put a sheet over because it hurts at night. And if you move at night, it just hurts, so you keep waking up” (P12, Garcia-Guillen et al., 2020, p. 18).
Sleep disruption can increase mood disorders, reduce quality of life and increase stress responsivity. Participants also felt they were a burden during a gout attack (Coulshed et al., 2020; Tatlock et al., 2017). “I can’t hack the pain, but I need to go pay these bills. And if I don’t hack the pain, and I don’t go to work, my family doesn’t eat” (P7, Lindsay et al., 2011, p.2). The ripple effect of a gout attack led to an inability to work, loss of income and economic burden for the participant and their family. In contrast, a few participants in less physically demanding jobs experienced less impact, as one stated, “No [it doesn’t affect my productivity], because I work with my head, not with my feet” (P15, Coulshed et al., 2020, p. 1375).
Most participants described forced lifestyle modifications. The severity of pain dictated the level of modification, specifically in terms of exercise, hobbies and travel (Li et al., 2022; Te Karu et al., 2013). “To go to the toilet, you’re crawling on the floor” (P1, Te Karu et al., 2013, p. 217). “I rely on my hands, and I can’t play the piano anymore … from the gout” (P2, Coulshed et al., 2020, p. 1376). In contrast, a small subset of participants reported no gout-related limitations between attacks (Coulshed et al., 2020; Ten Klooster et al., 2013). “When I’m not having an attack, I don’t notice my gout or arthritis at all” (P4, Ten Klooster et al., 2013, p. 4). This lack of noticing demonstrates the possibility of gout being optimally managed, which in turn improves quality of life. The most prominent emotional impact experienced by participants was continuous worry about impending gout flares (Coulshed et al., 2020; Kong et al., 2019). “…it’s like living in a little box that you’re just waiting when is the hurricane coming?” (P6, Kong et al., 2019, p. 3). This sense of waiting also affected self-esteem: “I’m disappointed with my body. I’m disappointed that I’m not free, that I could at any time get a gout attack” (P2, Coulshed et al., 2020, p. 1375). The inability to anticipate a gout attack affected the participants’ ability to feel they had control, and negatively affected their emotional well-being.
Theme 2: Misconceptions about gout
Narrative storyline – Misunderstanding and missed management
The second theme, misconceptions about gout, illuminates how participants navigate living with gout when surrounded by common misconceptions about it coming from themselves, the community and health practitioners. These negative misconceptions undermined their access to the best treatment. Participants’ narratives included preconceived notions about gout being self-inflicted or trivialised, and the permanence of a lesser quality of life (Seow et al., 2018; Te Karu et al., 2013). “You just accept it, don’t question.” (P4, Te Karu et al., 2013, p. 217). “I don’t regret [that] I can’t do this; I resigned to the fact [that] I have this problem” (P10, Seow et al., 2018, p. 61). “I don’t share all my sufferings, so I just take care of myself. I confine [it] within me” (P3, Seow et al., 2018, p. 61). These ways of thinking about living with gout contributed to misconceptions and delayed participants from seeking care.
Some participants believed gout was an unimportant, nuisance illness (Chandratre et al., 2015). “I don’t think it’s perceived to be life-threatening, whereas cancer and heart attacks are.” (P not identified, Chandratre et al., 2015, p. 1201). Another misperception that affected seeking treatment was that gout could not be treated (Lindsay et al., 2011). “I think I have accepted the fact that there is no cure, because I haven’t talked to anybody who has had it and says they don’t get it anymore.” (P7, Lindsay et al., 2011, p. 4).
Misunderstandings about gout between participants and their own family also contributed to suboptimal gout management, especially the idea that gout was self-inflicted (Richardson et al., 2015; Te Karu et al., 2013). “I thought it was all my fault” (P4, Te Karu et al., 2013, p. 218). “[Name] [wife] goes [expletive] nuts at me. She looks at me and says, ‘[Expletive] here we go again.’ ” (P9, Te Karu et al., 2013, p.218). Stigma also contributed to a sense of shame and embarrassment (Chandratre et al., 2015; Lindsay et al., 2011). “They asked me what was wrong with it, and I said, ‘Maybe I got poisoned’. They relate gout with all the negative stuff with it, it took me a long time to actually admit the fact that I did have this sickness” (P2, Lindsay et al., 2011, p. 4). Stigma creates an unnecessary sense of shame. Participants suggested that stereotyping and stigmatisation also originated from some health practitioners, influencing their reluctance to seek treatment (Coleman et al., 2021; Kong et al., 2019). “He [senior doctor] said, `What gives gout?’ The young fella [junior doctor] said, `Oh, too much rich living, too much rich food’. (P2, Kong et al., 2019, p. 4). “I’m only young, I’m not that old, and that’s what the surgeon said, at your age you shouldn’t have this disease” (P7, Kong et al., 2019, p. 4).
Participants felt some health practitioners saw gout as a nuisance illness and that some of them misunderstood the reality of gout (Te Karu et al., 2013). “These doctors need to have a bash of gout and see what it feels like to them, then they would see what it’s really like. I think they have no idea” (P9, Te Karu et al., 2013, p. 219). “I came here to see a doctor to find out whether my uric acid level and other data are normal. I had a lot of questions, but before I could ask, the doctor called the next patient and urged me to leave.” (P16, Li et al., 2022, p. 5). Some health practitioners may lack knowledge about the presentation of gout symptoms (Chandratre et al., 2015; Diaz-Torne et al., 2024; Liddle et al., 2015). “I went to the A&E […] I saw a doctor … he thought I’d been bitten on the foot. It was just really a shot in the dark, so my medical advice then was not geared towards gout.” (Henry, 63yrs, Liddle et al., 2015, p. 3).
Where health practitioners failed to provide good care to gout patients, whether from lack of knowledge or other reasons, this resulted in some participants living with pain for sustained periods of time without adequate management, and lacking understanding that gout is a treatable disease.
Theme 3: Finding a sense of agency
Narrative storyline – Negotiating life with gout
This theme highlights how participants navigate their pathway to self-management and develop a sense of agency in managing to live with gout. Some participants’ understanding of gout was limited to their own experience and what they observed from other “gout sufferers”. Other participants sought information from sources such as family members, nurses and other health professionals, educational resources and fellow participants (Howren et al., 2018; Li et al., 2022). “I did not know about gout until I was diagnosed with it. I just have joint pain and do not have any other symptoms of gout. But I saw the tophi and joint damage of other patients, I realised that gout is such a serious disease.” (P12, Li et al., 2022, p. 4).
Processing their feelings about the diagnosis of gout and understanding the disease are the first steps people need to take to navigate it. This understanding can lead to lifestyle choices that help them manage their own symptoms (Howren et al., 2018). For one patient, having gout was not too concerning, as he already had many other health issues. “I’ve got so many other things going on [health issues] … at the moment it, what’s one more little [gout], yeah, nothing to worry about” (P11, Kong et al., 2019). A diagnosis of gout brought a sense of relief to some participants who worried what the severe pain might mean. Some doubted the accuracy of their diagnosis (Liddle et al., 2015). “Main concern was that he [patient] was going to lose a toe basically, rather than it being gout, so he’s actually, if anything, relieved that it was gout as a diagnosis.” (GP 1, Kong et al., 2019, p. 4). “I often doubt, I think, ‘Oh have they got it wrong?’ You know, because I don’t speak to anybody who’s got it, especially my age, […] they’re not women”. (Georgina, 41yrs, Liddle et al., 2015, p. 4).
People who recognise the common traits of gout can adapt to living with it. This adaptation involves making lifestyle modifications, such as adjusting their diet, identifying personal triggers and making practical changes in clothing, as well as adapting to pain (Coulshed et al., 2020; Li et al., 2022). “Since I knew I had gout, I began to adjust my lifestyle, not staying up late, drinking less carbonated drinks, less alcohol, and not eating high purine foods” (P18, Li et al., 2022, p. 6). Some participants found that their gout-related diet changes had a positive impact on their health, although others found it harder to adapt (Li et al., 2022). “It is very painful not to eat seafood or drink. Because, after all, I have to attend some alcoholic drinking occasions … It is not easy to quit [alcoholic drinks].” (P17, Li et al., 2022, p. 6).
Some participants felt comfortable enough to adjust their diet and medication during an asymptomatic period (Howren et al., 2018). “Because I hadn’t been having flare-ups, I felt I could indulge a little bit more in some of the foods that I knew were triggers” (P8, Howren et al., 2018, p. 3). They felt empowered to try different things when they felt well, and being organised helped them to self-manage (Coulshed et al., 2020; Garcia-Guillen et al., 2020; Howren et al., 2018). “… my gout is part of my planning” (P3, Coulshed et al., 2020, p. 1375). “Well, I’m on other medications, so I’ve got a very regimented schedule when I take a medication.” (P1, Howren et al., 2018, p. 4). This participant made their medication regimen part of their daily routine.
Motivation to seek health care increased when participants felt a sense of agency in living with gout (Diaz-Torne et al., 2024; Howren et al., 2018). “That pain and discomfort that I had from gout was inhibiting. And so that was the main point that made me decide to seek treatment and knowledge on gout” (P2 Diaz-Torne et al., 2024, p.7). “If I don’t take my medication, I don’t want to get sick, right, because I’ve got to take care of my family and my husband and my housework too” (P3, Howren et al., 2018, p. 3). Taking control refers to the journey that participants undertake as they assume responsibility and become proactive in their self-management (Díaz-Torne et al., 2024; Howren et al., 2018). “I mean the bottom line is, I’m the patient and know my body so ultimately it becomes my responsibility” (P12, Howren et al., 2018, p. 3). “I’ve got one of those little kits that you use. I wanted to understand my own disease and manage my own disease, so I calibrated my monitor with the blood test. At some points, I titrated my own dose of Allopurinol” (Adam, 41yrs, Liddle et al., 2015, p.5).
Optimal management of gout is achievable with urate-lowering drug therapy. Participants who achieve medication adherence experience improved quality of life and a reduction in gout flares.
Discussion
This meta-synthesis endeavoured to journey with participants through their lived experiences with gout. Twenty studies on the reality and impact of living with gout were explored. The findings of this synthesis reveal the potentially devastating effects of poorly treated gout on every aspect of life.
The pain that disrupts lives is a dominating factor in participants’ accounts of living with gout. Therefore, optimal management must be a key focus. Management of pain in gout involves two key elements: managing acute flares and using urate-lowering drug therapy, which is the cornerstone of gout treatment. Evidence-based management guidelines, such as the 2020 American College of Rheumatology Guideline for the Management of Gout and the National Institute for Health and Care Excellence guidelines, should guide all health-care professionals in the optimal management of gout (Fitzgerald et al., 2020; NICE, 2022). These guidelines provide direction for clinicians and patients on managing acute gout flares and incorporating options for the individual complexities patients face in terms of their preferences, comorbidities and tolerances.
Approximately half those living with chronic illness experience stigma. Stigma may be internalised and anticipated personally, as well as experienced in health-care and social contexts (Earnshaw & Quinn, 2011; Pearl et al., 2024). Stigma can involve negative stereotyping, being labelled as different, separation and discrimination. In any form, it poses a barrier to optimal management of chronic disease (Link & Phelan, 2001; Pearl et al., 2024). Internalised stigma creates a barrier to accessing health care, as the person believes they do not deserve care. Patients with chronic illness can experience stigma in the health service, if the health professional believes the person is to blame for their poor health, leaving them with the feeling that they are a nuisance and that the health practitioner is frustrated with them (Pearl et al., 2024).
The stigma associated with gout has a significant influence on whether people seek help to manage their condition, and also affects practitioners’ treatment of gout. One source of stigma can be the unhelpful attitudes and myths about gout within families and the community (Liddle et al., 2015). Stigma is a barrier to a person receiving timely and appropriate medical care for their gout — and withoutf urate-lowering therapy, this can lead to them suffering constant gout (Liddle et al., 2015). Distorted perceptions of the nature of gout have a marked negative effect on patients’ attitudes to their condition and its treatment (Doherty et al., 2012). Poor knowledge about gout and lack of interest among doctors also negatively affects health outcomes (Doherty et al., 2012). The well-being of individuals and populations can improve by lessening the stigma attached to gout. De-stigmatisation efforts can include the dissemination of knowledge by medical experts, cultural advocates and the media, publicly advocating for the worth of people with gout, and removing blame. Reducing stigma requires transforming beliefs and behaviours among individuals, the public and the health sector (Clair et al., 2016).
Having a sense of agency can involve feeling empowered to make choices and manage the consequences (Moore, 2016). Chronic conditions, although each unique in their pathology, share management challenges. Individuals can improve their health by developing skills to take responsibility for the daily management of their own chronic condition. Self-management programmes can equip individuals with these skills (Grady & Gough, 2014). Nurses are central members of the multidisciplinary team supporting people with long-term conditions. Their role in helping people with gout to develop a self-managing toolkit involves developing a partnership with the individual, their family and their community, as well as following a systematic, individualised approach with each person (Dineen-Griffin et al., 2019). Nurse-led, individually focused care, involving education and disease management, improves long-term adherence to treatment, potentially reducing gout flares (Fuller et al., 2020). Further research is needed to assess the impact of nurse-led services on improving quality of life and well-being for people with gout, given that the prevalence of gout in New Zealand is among the highest internationally.
Recommendations
Best outcomes for gout patients require a multifaceted, patient-centred approach, incorporating education methods that align with the patient’s preferences and health literacy (van Onna et al., 2014). This approach requires identifying the gaps in the patient’s knowledge and barriers to treatment. A multidisciplinary team approach to care is best, including nurse-led and marae-based strategies, with cultural supports to ensure effective communication and education. For patients to successfully manage their own condition, they need effective education (Fields & Batterman, 2018). This leads to optimal disease management and fosters a sense of agency in the person living with gout. Recommendations from the findings of this review include:
- Referrals to rheumatologists from primary care should be timely so patients can live well with gout and manage complications that may affect their daily activities.
- Education on gout for health-care providers is needed. The Gout Guide NZ is a dynamic, must-have resource for GPs, nurses, pharmacists, health coaches and all health-care teams in Aotearoa New Zealand.
- De-stigmatise gout by improving health literacy and raising awareness of gout as a chronic condition. Clinics should display A4 posters — gout is more than a pain in the toe. Patient and whānau resources, such as information booklets and postcards with information about educational videos, should be readily available. (In New Zealand, these are available from Gout Guide NZ and Arthritis NZ.) To improve the quality of life of this expanding population, a better understanding of the stigma attached to chronic illness in health services will be increasingly important.
- Patients and their families should have access to multi-disciplinary care, via nurse-led gout clinics. Raising awareness of the diversity of people living with gout should improve cultural awareness and decrease stigma attached to the condition.
- Gout management may improve if uric acid targets were included in the national health targets, and gout was specifically included as an aspect of formal qualification in the education of health-care practitioners.
Limitations
This meta-synthesis sheds light on the experiences of individuals with gout. However, only qualitative studies were included in this review. Quantitative studies may enable a broader understanding through measuring experience, eg cohort studies that show the trajectory of gout and its impact on function.
Conclusion
This meta-ethnography identified and synthesised the findings of 20 qualitative studies on the lived experience of people with gout. Storylines evolved from these studies, which demonstrated the ripple effect that pain from gout flares has on an individual’s quality of life. The studies shed light on the trials and tribulations of navigating life with gout, while surrounded by misconceptions and negative stigmas, and on the way people with gout can achieve self-management through learning about their condition. A potentially debilitating disease such as gout does not have to be tolerated in silent suffering and stoicism. These powerful and vulnerable narratives enable us to briefly envision what it means to walk a mile in someone’s shoes, living with gout as a long-term condition. There are ways for people with gout to significantly improve their quality of life through effective self-management of the condition, and nurses play a key role in this.
References
Afzal, M., Rednam, M., Gujurathi, R., & Widrich, J. (2025). Gout. StatPearls.
Benn, C. L., Dua, P., Gurrell, R., Loudon, P., Pike, A., Storer, R. I., & Vangjeli, C. (2018). Physiology of Hyperuricemia and Urate-Lowering Treatments. Frontiers in Medicine, 5.
BPAC NZ. (2021). Managing gout in primary care.
Chandratre, P., Mallen, C. D., Roddy, E., Liddle, J., & Richardson, J. (2015). “You want to get on with the rest of your life”: a qualitative study of health-related quality of life in gout. Clinical Rheumatology, 35(5), 1197–1205.
Chang, E., & Johnson, A. (2018). Living with chronic illness and disability: principles for nursing practice (3rd ed.). Elsevier Australia.
Clair, M., Daniel, C., & Lamont, M. (2016). Destigmatization and health: Cultural constructions and the long-term reduction of stigma. Social Science & Medicine, 165, 223–232.
Coleman, W., Spencer, D., Wong, P., & Manolios, N. (2021). An enquiry into the crippling gout affecting Pacific Islander and Māori men in Western Sydney. International Journal of Rheumatic Diseases, 24(11), 1394-1401.
Coulshed, A., Nguyen, A. D., Stocker, S. L., & Day, R. O. (2020). Australian patient perspectives on the impact of gout. International Journal of Rheumatic Diseases, 23(10), 1372–1378.
Dalbeth, N., Choi, H. K., Joosten, L. A. B., Khanna, P. P., Matsuo, H., Perez-Ruiz, F., & Stamp, L. K. (2019). Gout. Nature Reviews Disease Primers, 5(1).
Dalbeth, N., Dowell, T., Gerard, C., Gow, P., Jackson, G., Shuker, C., & Te Karu, L. (2018). Gout in Aotearoa New Zealand: The equity crisis continues in plain sight. New Zealand Medical Journal, 131(1485).
Dalbeth, N., Merriman, T. R., & Stamp, L. K. (2016). Gout. The Lancet, 388(10055), 2039–2052.
Dalbeth, N., Winnard, D., Gow, P., Boswell, R., Karu, L., Lindsay, K., Arroll, B., & Stamp, L. (2015). Urate testing in gout: why, when and how. New Zealand Medical Journal, 128(1420).
Dehlin, M., Jacobsson, L., & Roddy, E. (2020). Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nature Reviews Rheumatology, 16(7), 380–390.
Diaz-Torne, C., Pou, M. A., Horne, A., Gasteiger, C., & Dalbeth, N. (2024). “Gout was like the boss”. A qualitative study exploring the impact of gout on employment. RMD Open, 10(3), e004443–e004443.
Dineen-Griffin, S., Garcia-Cardenas, V., Williams, K., & Benrimoj, S. I. (2019). Helping patients help themselves: A systematic review of self-management support strategies in primary health care practice. PLoS One, 14(8).
Doherty, M., Jansen, T. L., Nuki, G., Pascual, E., Perez-Ruiz, F., Punzi, L., So, A. K., & Bardin, T. (2012). Gout: why is this curable disease so seldom cured? Annals of the Rheumatic Diseases, 71(11), 1765–1770.
Earnshaw, V. A., & Quinn, D. M. (2011). The Impact of Stigma in Healthcare on People Living with Chronic Illnesses. Journal of Health Psychology, 17(2), 157–168.
Fields, T. R., & Batterman, A. (2018). How Can We Improve Disease Education in People with Gout? Current Rheumatology Reports, 20(3).
Fitzgerald, J., Dalbeth, N., Mikuls, T., Brignardello-Petersen, R., Guyatt, G., Abeles, A., Gelber, A., Harrold, L., Khanna, D., King, C., Levy, G., Libbey, C., Mount, D., Pillinger, M., Rosenthal, A., Singh, J., Sims, J., Smith, B., Wenger, N., & Sangmee, S. (2020). 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care & Research, 72(6), 744–760.
France, E. F., Cunningham, M., Ring, N., Uny, I., Duncan, E. A. S., Jepson, R. G., Maxwell, M., Roberts, R. J., Turley, R. L., Booth, A., Britten, N., Flemming, K., Gallagher, I., Garside, R., Hannes, K., Lewin, S., Noblit, G. W., Pope, C., Thomas, J., & Vanstone, M. (2019). Improving reporting of meta-ethnography: the eMERGe reporting guidance. BMC Medical Research Methodology, 19(1).
France, E. F., Ring, N., Noyes, J., Maxwell, M., Jepson, R., Duncan, E., Turley, R., Jones, D., & Uny, I. (2015). Protocol-developing meta-ethnography reporting guidelines (eMERGe). BMC Medical Research Methodology, 15(1).
France, E. F., Uny, I., Ring, N., Turley, R. L., Maxwell, M., Duncan, E. A. S., Jepson, R. G., Roberts, R. J., & Noyes, J. (2019). A methodological systematic review of meta-ethnography conduct to articulate the complex analytical phases. BMC Medical Research Methodology, 19(1).
Frecklington, M., Williams, A., Dalbeth, N., McNair, P., Gow, P., & Rome, K. (2019). The footwear experiences of people with gout: a qualitative study. Journal of Foot and Ankle Research, 12(1).
Fuller, A., Jenkins, W., Doherty, M., & Abhishek, A. (2020). Nurse-led care is preferred over GP-led care of gout and improves gout outcomes: results of Nottingham Gout Treatment Trial follow-up study. Rheumatology, 59(3), 575-579.
Galassi, F. M., Ingaliso, L., Papa, V., Lorenzi, R., Percivaldi, E., & Varotto, E. (2024). On the early uses of the word “gout”: novel evidence and a critical assessment of the published literature. Reumatismo, 76(2).
Garcia-Guillen, A., Stewart, S., Su, I., Taylor, W. J., Gaffo, A. L., Gott, M., Slark, J., Horne, A., & Dalbeth, N. (2020). Gout flare severity from the patient perspective: a qualitative interview study. Arthritis Care & Research, 74(2), 317-323.
Gill, I., Dalbeth, N., Ofanoa, M., & Goodyear-Smith, F. (2020). Interventions to improve uptake of urate-lowering therapy in patients with gout: a systematic review. BJGP Open, 4(3), bjgpopen20X101051.
Grady, P. A., & Gough, L. L. (2014). Self-Management: A comprehensive approach to management of chronic conditions. American Journal of Public Health, 104(8), 25-31.
Health Quality & Safety Commission. (2018). Māori and Pacific peoples more likely to suffer from gout, less likely to be treated.
Health Quality & Safety Commission. (2019). Gout.
Howren, A., Cox, S. M., Shojania, K., Rai, S. K., Choi, H. K., & De Vera, M. A. (2018). How patients with gout become engaged in disease management. Arthritis Research and Therapy, 20(1), 110.
Kong, D. C. L., Sturgiss, E. A., Raj, A. K. D., & Fallon, K. (2019). What factors contribute to uncontrolled gout and hospital admission? A qualitative study of inpatients and their primary care practitioners. BMJ Open, 9(12), e033726.
Kuo, C.-F., Grainge, M. J., Zhang, W., & Doherty, M. (2015). Global epidemiology of gout: prevalence, incidence and risk factors. Nature Reviews Rheumatology, 11(11), 649-662.
Li, Q., Liu, T., Zhang, S., & Miao, X. (2022). Illness perception and treatment experience in patients with gout: a descriptive qualitative study. Clinical Rheumatology, 41, 1185-1195.
Liddle, J., Roddy, E., Mallen, C. D., Hider, S. L., Prinjha, S., Ziebland, S., & Richardson, J. C. (2015). Mapping patients’ experiences from initial symptoms to gout diagnosis. BMJ Open, 5(9).
Lindsay, K., Gow, P., Vanderpyl, J., Logo, P., & Dalbeth, N. (2011). The Experience and Impact of Living With Gout. Journal of Clinical Rheumatology, 17(1), 1-6.
Link, B. G., & Phelan, J. C. (2001). Conceptualizing Stigma. Annual Review of Sociology, 27(1), 363-385.
Moore, J. W. (2016). What Is the Sense of Agency and Why Does it Matter? Frontiers in Psychology, 7(1272).
Morris, C., Macdonald, L., Stubbe, M., & Dowell, A. (2016). “It’s complicated” — talking about gout medicines in primary care consultations: a qualitative study. BMC Family Practice, 17(1).
National Institute for Health and Care Excellence (NICE). (2022). Gout: diagnosis and management (NICE guideline).
Noblit, G. W., & Hare, R. D. (1988). Meta-Ethnography: synthesizing qualitative studies. Sage.
Nolte, E. (2008). Caring for people with chronic conditions: A health system perspective. Open University Press.
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., & McGuinness, L. A. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Systematic Reviews, 10(1).
Pearl, R. L., Li, Y., Groshon, L. C., Hernandez, M., Saunders, D., Sheynblyum, M., Driscoll, K. A., Gelfand, J. M., Manavalan, P., Montanez-Wiscovich, M., Pereira, D. B., Puhl, R. M., Wadden, T. A., Waxenberg, L. B., Westen, S. C., & Lou, X.-Y. (2024). Measuring internalized health-related stigma across health conditions: development and validation of the I-HEARTS Scale. BMC Medicine, 22(1).
Porritt, K., Evans, C. Bennett, C., Loveday, H., Bjerrum, M., Salmond, S., Munn, Z., Pollock, D., Pang, D., Vineetha, K., Seah, B., & Lockwood, C. (2024). Systematic reviews of qualitative evidence. In E. Aromataris, C. Lockwood, K. Porritt, B. Pilla, & Z. Jordan (Ed.). JBI Manual for Evidence Synthesis. JBI.
Ragab, G., Elshahaly, M., & Bardin, T. (2017). Gout: An old disease in new perspective. Journal of Advanced Research, 8(5), 495-511.
Regan-Smith, M., Hirschmann, K., Iobst, W., & Battersby, M. (2022). Teaching residents chronic disease management using the Flinders model. LVHN Scholarly Works.
Richardson, J. C., Liddle, J., Mallen, C. D., Roddy, E., Prinjha, S., Ziebland, S., & Hider, S. (2015). “Why me? I don’t fit the mould … I am a freak of nature”: A qualitative study of women’s experience of gout. BMC Women’s Health, 15(1).
Rimler, E., Lom, J., Higdon, J., Cosco, D., & Jones, D. (2016). A Primary Care Perspective on Gout. Open Urology & Nephrology Journal, 9(1), 27-34.
Rolston, C. J., Conner, T. S., Stamp, L. K., Neha, T., Pitama, S., Fanning, N., Janes, R., Judd, A., Hudson, B., Hegarty, R. M., & Treharne, G. J. (2018). Improving gout education from patients’ perspectives: A focus group study of Māori and Pākehā people with gout. Journal of Primary Health Care, 10(3), 194.
Sattar, R., Lawton, R., Panagioti, M., & Johnson, J. (2021). Meta-ethnography in healthcare research: A guide to using a meta-ethnographic approach for literature synthesis. BMC Health Services Research, 21(1).
Seow, L. L., Jiao, N., Wang, W., Holroyd, E., Teng, G. G., & He, H.-G. (2018). A Qualitative Study Exploring Perceptions of Patients With Gout. Clinical Nursing Research, 29(1), 56-65.
Singh, J. A. (2014). Facilitators and barriers to adherence to urate-lowering therapy in African-Americans with gout: A qualitative study. Arthritis Research & Therapy, 16(2), R82.
Sivera, F., Andres, M., & Dalbeth, N. (2022). A glance into the future of gout. Therapeutic Advances in Musculoskeletal Disease, 14.
Smith, H. S., Bracken, D., & Smith, J. M. (2011). Gout: Current Insights and Future Perspectives. Journal of Pain, 12(11), 1113-1129.
Smith, N., Karakashian, A. L., & Pravikoff, D. (2018). Gout. Coursehero.com.
Tatlock, S., Rüdell, K., Panter, C., Arbuckle, R., Harrold, L. R., Taylor, W. J., & Symonds, T. (2017). What Outcomes are Important for Gout Patients? In-Depth Qualitative Research into the Gout Patient Experience to Determine Optimal Endpoints for Evaluating Therapeutic Interventions. The Patient, 10(1), 65-79.
Te Karu, L., Bryant, L., & Raina Elley, C. (2013). Māori experiences and perceptions of gout and its treatment: A kaupapa Māori qualitative study. Journal of Primary Health Care, 5(3), 214.
ten Klooster, P. M., Vonkeman, H. E., Oude Voshaar, M. A. H., Bode, C., & van de Laar, M. A. F. J. (2013). Experiences of gout-related disability from the patients’ perspective: A mixed methods study. Clinical Rheumatology, 33(8), 1145-1154.
van Onna, M., Hinsenveld, E., de Vries, H., & Boonen, A. (2014). Health literacy in patients dealing with gout: A qualitative study. Clinical Rheumatology, 34(9), 1599-1603.
Wertheimer, A., Morlock, R., & Becker, M. A. (2013). A Revised Estimate of the Burden of Illness of Gout. Current Therapeutic Research Clinical and Experimental, 75(75), 1-4.
Supplementary File 1. Search strings
| Search # | Field tag | CINAHL |
|---|---|---|
| 1 | Title or abstract | Adult* OR elderly OR age* OR “old person” OR “middle age*” OR senior OR “young adult*” |
| 2 | Main Heading (MH) | Adult OR frail elderly OR “young adult” |
| 3 | S1 OR S2 | |
| 4 | Title or abstract | Experience* OR “lived experience*” OR “patient experience*” OR “personal experience*” OR perception* OR thought* OR feeling* OR opinion* OR belief* OR “life experience*” Or “attitude* to illness” OR emotion* |
| 5 | Main Heading (MH) | |
| 6 | S4 or S5 | |
| 7 | Title or abstract | |
| 8 | Main Heading (MH) | |
| 9 | S7 OR S8 | |
| 10 | S3 AND S6 AND S9 | |
| Filters | No date filter, remove full text limiter |
Supplementary File 2. Critical appraisal of the included studies
NOTES
Quality appraisal tool questions:
- Congruity between the stated philosophical perspective and the research methodology;
- Congruity between the research methodology and the research question or objectives;
- Congruity between the research methodology and the methods used to collect data;
- Congruity between the research methodology and the representation and analysis of data;
- There is congruence between the research methodology and the interpretation of results;
- Locating the researcher culturally or theoretically;
- Influence of the researcher on the research, and vice-versa, is addressed;
- Representation of participants and their voices;
- Ethical approval by an appropriate body;
- Relationship of conclusions to analysis, or interpretation of the data.
Dependability was scored by the number of “yes” votes for questions 2, 3, 4, 6 and 7; can be scored overall as High, Moderate, Low or Very low (Munn et al., 2014).
Daily doses – uncut news
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


