
About the authors:Sarah Gilbertson is a clinical nurse specialist in neurology at Waikato district – Te Manawa Taki, Te Whatu Ora – Health New Zealand. Author contributions: This article was accepted for publication in September 2024. |
ABSTRACTBackground: Epilepsy poses challenges in both treatment and daily life due to unpredictable seizures and the side effects of associated treatment. Adversities and comorbidities have a negative effect on well-being. Behaviour therapy has shown promise in enhancing self-management and well-being across various long-term conditions. Aim: This integrative review aimed to identify whether behaviour therapy improves well-being in adults living with epilepsy. Methods: An integrative review was undertaken using databases including MEDLINE Complete, Pubmed, CINAHL Complete, Science Direct, Clinical Key, PsycINFO, GALE Health & Wellness and GALE Academic. Studies published in English, using quantitative and qualitative methodologies, and presenting primary data analysis on the impact of behaviour therapy on the well-being of adults living with epilepsy were included in the review. Findings: Sixteen studies were included in the review. Three themes emerged from the synthesis. Quantitative data from all studies demonstrated improvements in well-being. Barriers to adults living with epilepsy participating in and completing behaviour therapy varied, including transportation challenges, memory problems, and issues with technology literacy. Conclusion: Although behaviour therapy was found to improve well-being in some people living with epilepsy, there are significant limitations in generalising the findings of this review to people living with epilepsy in New Zealand. |
||
KEYWORDS |
|||


INTRODUCTION
EPILEPSY IS A COMMON long-term neurological condition that can be challenging to treat and even more challenging to live with. Seizures can be unpredictable, and treatment is often associated with side effects. The adversities and comorbidities associated with epilepsy are well known to affect well-being negatively. Various behaviour therapy interventions help improve self-management and well-being in people living with various long-term conditions. This integrative review aimed to identify whether behaviour therapy improves well-being in adults living with epilepsy.
BACKGROUND
The World Health Organization estimates there are 50 million global cases of epilepsy, predominantly in low- to middle-income countries. In New Zealand, 45,000 to 50,000 individuals live with epilepsy, with 2000 new diagnoses annually. Characterised by “an enduring predisposition to generate epileptic seizures” (Fisher, 2014, p. 476), epilepsy involves brief, involuntary episodes from abnormal neuronal activity, impacting daily life. Seizures can compromise well-being, affecting employment, education, and daily activities. Due to the nature of epilepsy, self management is an essential component in achieving and maintaining well-being (Banks, 2021), but well-being affects the ability of a person to be able to
self-manage.
Behaviour therapy is effective in managing long-term conditions, and
enhancing well-being, especially with comorbidities like depression and anxiety (Hofmann, 2021; Chan et al., 2016; Egan et al., 2015). It employs a client-centred,
problem-focused approach, actively engaging individuals in goal-setting and behaviour change, with therapists providing education and support (Spiegler,
2016). With a diverse history since the 1920s, including variations like cognitive
behavioural therapy and mindfulness, behaviour therapy offers a structured approach addressing cognitive processes, emotions, and behaviour modification
(Blackwell & Heidenreich, 2021). Its evidence-based nature aligns with factors
influencing well-being, suggesting its potential to improve well-being, especially in conditions like epilepsy (Cuijpers et al., 2008; Centers for Disease Control and Prevention, 2018).
Given the prevalence and long-term nature of epilepsy, along with its complex management, the objective of this integrative review was to report the impact of behavioural therapy interventions on the well-being of adults with epilepsy. This review will enable us to make recommendations to inform decision-making in current health practices and policies. The review question was: “In adults living with epilepsy, does behaviour therapy improve well-being?”
METHODOLOGY
Study design
This study followed Toronto’s (2020) methodology for integrative review. An integrative review systematically and rigorously explores a phenomenon of interest in published literature, and can be used to guide evidence-based practice.
There are six steps when conducting an integrative review (Toronto, 2020):
-
- Formulate purpose and/or review question(s)
- Systematically search and select literature
- Quality appraisal
- Analysis and synthesis
- Discussion and conclusion
- Dissemination of findings
Formulate purpose and/or review questions
A review question was developed based on PICo (population, intervention, comparative outcome). Elements of PICo were identified, and the population was viewed as adults living with epilepsy; the intervention was behaviour therapy, and the comparative outcome was well-being. The PICO is presented in
Table 1 .
Table 1. PICo
| Population | Adults living with epilepsy | Adults living with epilepsy, either self-reported, as per the International League Against Epilepsy (ILAE) definition or as diagnosed by a neurologist. |
| Intervention | Behaviour therapy | Studies which used behaviour therapy interventions. There are a range of interventions that fall under the behaviour therapy umbrella so descriptions of interventions needed to be based on behaviour therapy. |
| Comparison and outcome | Well-being | Well-being needed to be assessed before and after the intervention to identify any changes. The term well-being is used synonymously with quality of life in this review. |
The inclusion and exclusion criteria for the review are shown in Table 2.
Table 2. Study search eligibility criteria
| Population | Adults living with epilepsy | Children |
| Intervention | Behaviour therapy | |
| Outcomes | Well-being or quality of life | |
| Types of studies | Primary research which included well-being or quality of life data in the outcomes | |
| Quality assessment | JBI checklists for randomised controlled trials and quasi-experimental studies | |
| Date limits | 2012-2022 | Prior to 2012 |
Literature search
A systematic search was carried out using the terms derived from the PICo. This search was undertaken using the following databases: MEDLINE Complete, Pubmed, CINAHL Complete, Science Direct, Clinical Key, PsycINFO, GALE Health & Wellness and GALE Academic. The inclusion criteria for this integrative review included: primary research studies where participants were exposed to behaviour therapy, research published from 2012-2022, and well-being assessed at baseline and following the intervention. Additional relevant articles were handpicked from the reference lists of secondary research studies. The PRISMA process diagram (Figure 1) identifies the studies selected at each stage.
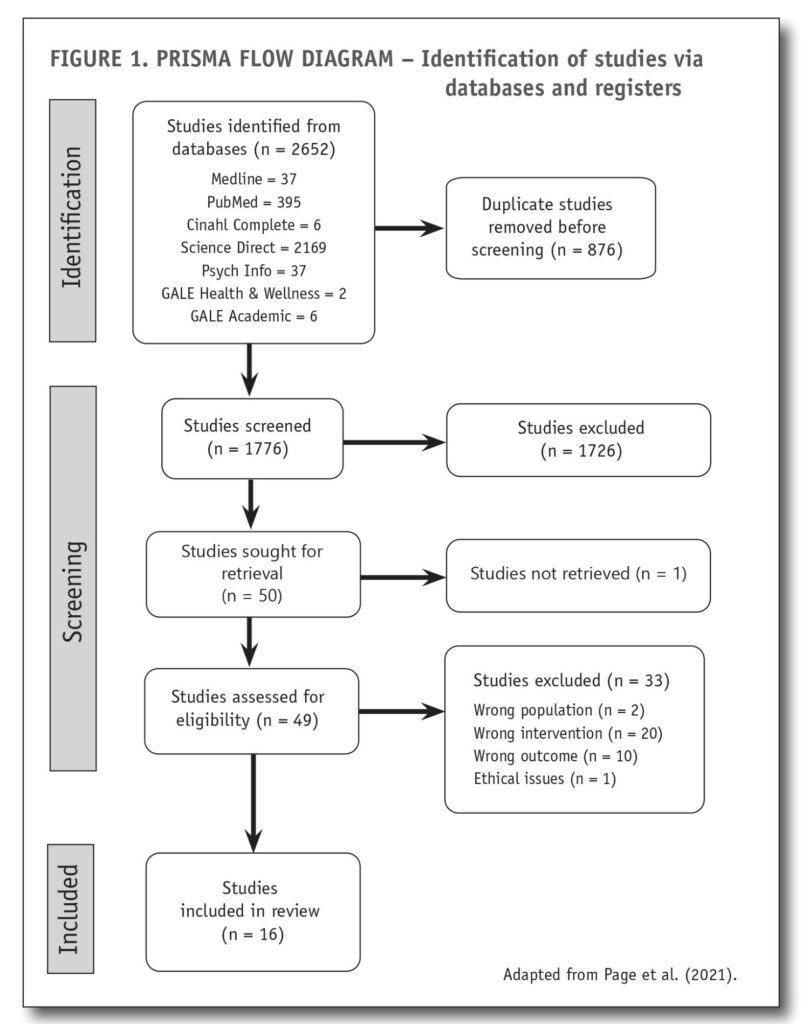
Search results
The search yielded 2652 records, of which 876 were removed, some being duplicates and some deemed irrelevant by title alone. The titles and abstracts of 1776 studies were screened, and full texts were obtained for 51 studies. These were loaded in the Covidence systematic review manager to review against the inclusion and exclusion criteria. The screening process led to 17 studies being identified as relevant for this review and to be assessed for quality. Two studies were excluded based on population criteria, 20 studies were excluded based on intervention criteria and 10 studies were excluded based on insufficient information on the effect of the intervention on well-being. This process is summarised in the PRISMA flow chart in Figure 1.
Quality appraisal
Each study was critically appraised for methodological quality, using the relevant Joanna Briggs Institute (JBI, 2020) critical appraisal tools for primary research studies. One study by Dewhurst et al. (2015) met all the inclusion criteria and so was initially included in this review, but was later excluded based on the lack of ethical considerations reported in the study. This appraisal led to 16 studies being included for analysis.
ANALYSIS AND SYNTHESIS
Qualitative and quantitative data were extracted from each study and collated into tables. The studies used in this review did not examine well-being in isolation but also examined other aspects of quality of life, such as insomnia and depression. Review matrixes were created to organise the data into tables. This process allows the reviewer to assimilate information, compare findings from all sources, and identify patterns and themes (Dwyer, 2020).
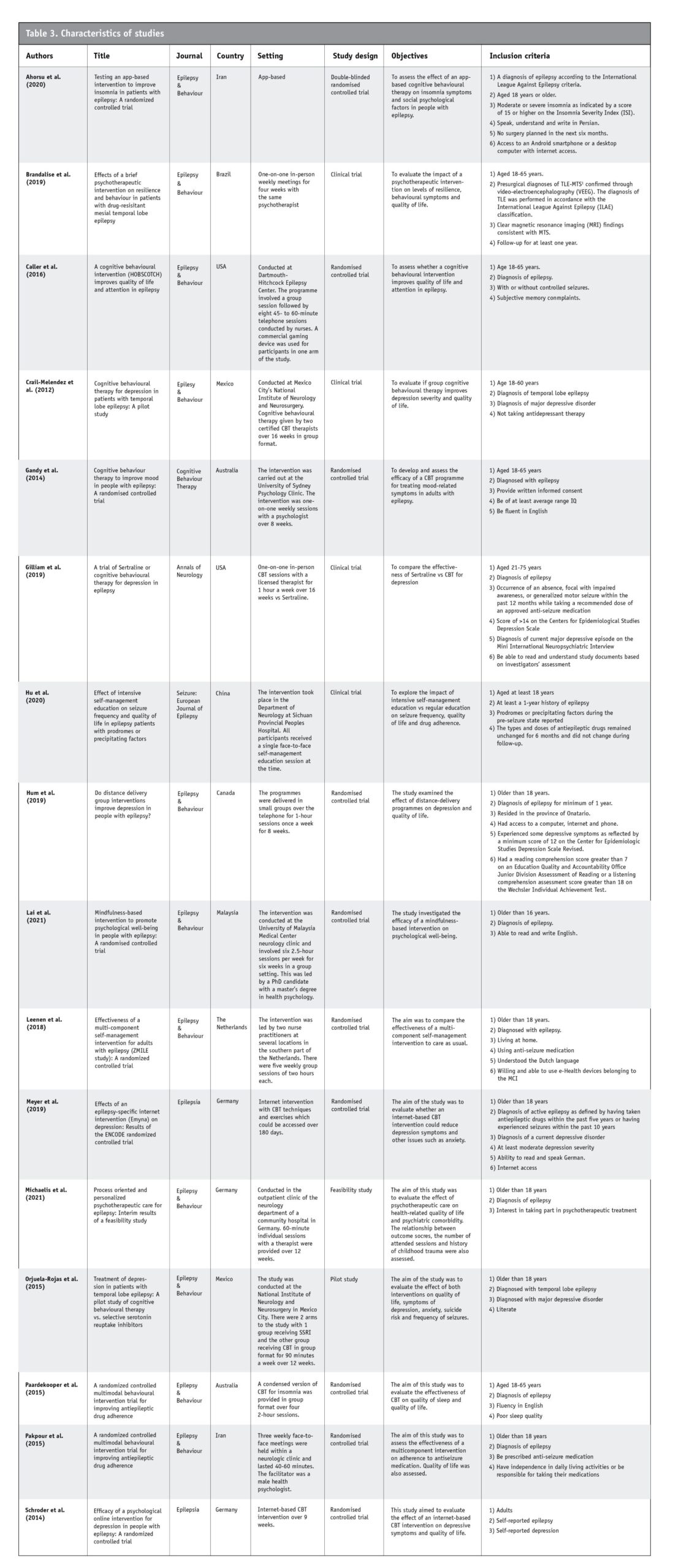
Characteristics of the studies
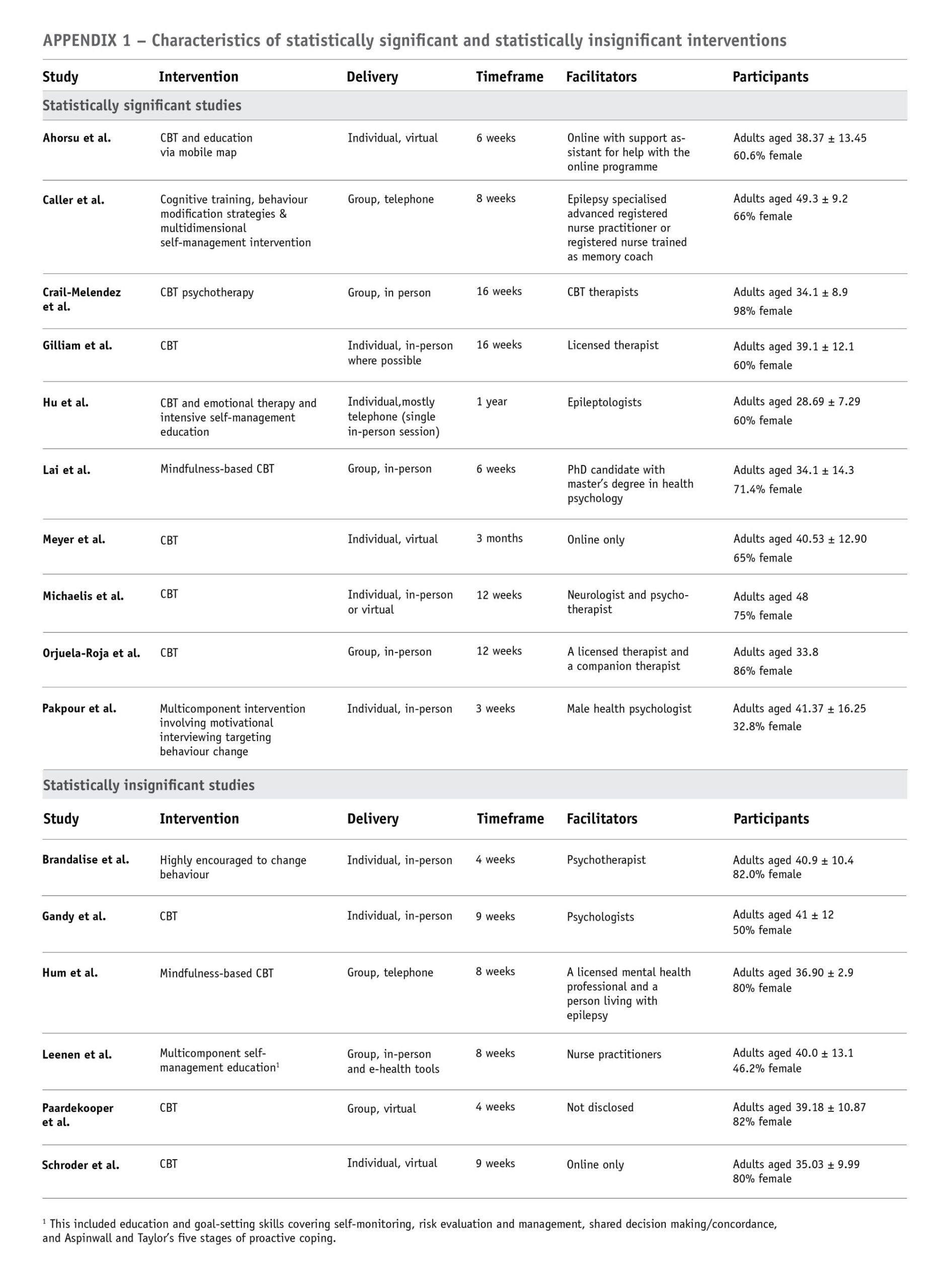
The characteristics of the studies are shown in Table 3 (below). Studies were carried out globally, but none were conducted in New Zealand. Most studies were conducted in Germany (n=3), and the remainder were from Iran (n=2), Mexico (n=2), USA (n=2), Australia (n=2), China (n=1), Canada (n=1), Malaysia (n=1) and The Netherlands (n=1). The interventions varied between studies, with some studies using cognitive behaviour therapy, some using multicomponent self-management education with behaviour modification strategies, one using mindfulness alone, and one using behaviour change with a psychotherapist. The duration of interventions varied greatly, ranging from three weeks to one year. There were a variety of settings, with some studies providing interventions virtually and some being carried out in person. Some interventions were carried out in group settings, and others were one-on-one. All of the studies used questionnaires before and after interventions, and some studies also provided qualitative data. The participants’ mean ages ranged from 28.69 years to 49.3 years. All of the studies had more female than male participants except for Gandy et al. (2014), where 50 per cent of participants were female; Leenen et al. (2018), where 46.2 per cent were female; and Pakpour et al. (2015), where 32.8 per cent were female.
Before and after well-being test scores were assessed to identify which studies achieved a statistically significant improvement in well-being following behaviour therapy. A review matrix was created to identify any themes that may characterise statistically significant or statistically insignificant studies (see Appendix 1). Qualitative and quantitative data related to well-being or quality of life were used in this review and are shown in Appendix 2. This table also includes limitations to identify any similarities between limitations. Each review matrix was analysed to identify themes, and this process was guided by three questions that were closely aligned with the review purpose:
- What was the effect of behaviour therapy on well-being in adults living with epilepsy?
- Identify any participant feedback/qualitative data on how the intervention affected well-being.
- Identify which studies showed a statistically significant improvement in well-being.
- Were there any similar characteristics between studies deemed to improve well-being?
- Type of behavioural intervention
- Duration of intervention
- Mode and delivery of the intervention
- Characteristics of the participants
- Was behaviour therapy an acceptable intervention?
- Identify any characteristics that were considered acceptable or unacceptable.
- Consider participation and/or completion of the intervention
FINDINGS
Three primary themes emerged from the synthesis: 1) the effects of behaviour therapy interventions on well-being, 2) common characteristics between studies deemed to improve well-being, and 3) the acceptability of the interventions.
Theme 1: Effect of behaviour therapy interventions on well-being
There were no qualitative data available on the effect of behaviour therapy on well-being in adults living with epilepsy. Quantitative data on the effect of behaviour therapy on well-being in adults living with epilepsy were available for every study included in this review. Nurses need to have an understanding of quantitative data but do not usually need to be fluent in statistics (Schroeder et al., 2022). Nurses usually either work with a statistician or receive formal training in statistics to avoid analytic errors (Grove & Cipher, 2017). The values used to examine statistical significance and change in well-being before and after interventions are p-values and t-tests. P-values indicate whether data is statistically significant or occurred by chance, and are important when measuring the quantitative outcome of research. A p-value of 0.05 or less means that there is a 5 per cent or less probability that the results may have occurred by chance and p-values of 0.05 or less are deemed statistically significant (Harvey & Land, 2022). T-tests are used to investigate the difference between samples with a distance from 0, whether positive or negative, providing a value to the difference (Grove & Cipher, 2017). Some t-test calculating tools are available online and were used in this review. Using t-tests and p-values, it was possible to calculate which studies produced statistically significant improvements in well-being.
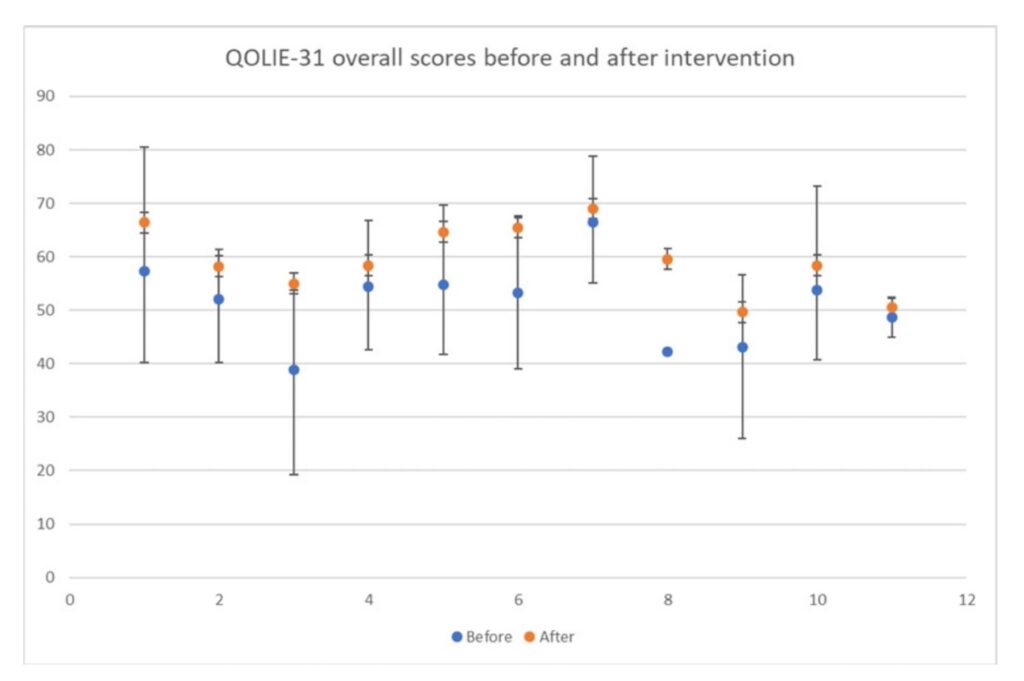
The studies included in this review used a variety of tools to assess well-being, with the Quality of Life in Epilepsy (QOLIE) inventories being the tools most commonly used. The QOLIE Development Group (1993) developed the QOLIE-89, QOLIE-31 and QOLIE-10, based on analysis of data obtained from people living with epilepsy in the United States. The QOLIE-89 contains 17 multi-item measures, while the QOLIE-31 and QOLIE-10 are shorter forms of the QOLIE-89. The QOLIE-89 takes up to 45 minutes to complete, the QOLIE-31 about 10 minutes to complete and the QOLIE-10 takes about two to three minutes (Jones et al., 2020). These questionnaires cover several domains, including emotional well-being, social functioning, energy/fatigue, cognitive functioning, seizure worry, medication effects and overall quality of life (Vickrey et al., 1993). Overall scores are obtained using a weighted average; overall score values can range from 0 to 100, with higher values reflecting better quality of life. Thirteen studies used the QOLIE-31, one study used QOLIE-89 and one study used QOLIE-10. Meyer et al. (2019) used the QOLIE-10 and found a statistically significant improvement in QOLIE-10 scores after the intervention. Gilliam et al. (2019) used the QOLIE-89 and also found a statistically significant improvement in quality of life after the intervention.
Although Brandalise et al. (2019) used the QOLIE-31 inventory, the overall scores differed considerably from the other studies that used the same tool and were also higher than the scores the QOLIE-31 can achieve. The overall QOLIE-31 score is meant to range from 0 to 100; however Brandalise et al’s pre-intervention mean overall QOLIE-31 score was 181.29 and the mean overall post-intervention score 191.12. The authors do not discuss why the overall QOLIE-31 scores do not fall between 0 and 100 but it is possible that they used raw scores rather than the recommended weighted scoring.
WHOQOL-BREF was used by Hum et al. (2019) and Schroder et al. (2014), who used this tool as well as QOLIE-31. WHOQOL BREF is an abbreviated version of the World Health Organization Quality of Life assessment tool which was developed to increase focus on quality of life and well-being (Programme on Mental Health World Health Organization, 1996). This tool covers four domains, including physical health, psychological, social relationships and environment, and was developed through research in centres around the world. Higher scores are associated with a better quality of life. Hum et al. (2019) identified a significant improvement in WHOQOL-BREF scores following the behavioural change intervention. While both Hum et al. (2019) and Schroder et al. (2014) identified improvements in WHOQOL-BREF scores after the intervention, the improvement was not enough to achieve statistical significance.
In studies with small sample sizes, there needs to be a greater improvement in pre- and post-intervention scores for results to be statistically significant (Peacock & Peacock, 2011). Due to the small sample sizes of the studies used in this review, statistically significant results were difficult to achieve. Ten of the 16 studies found a statistically significant improvement in well-being in people living with epilepsy following behaviour therapy. The t-tests comparing pre- and post-intervention well-being scores showed a statistically significant improvement, with the p-value for the t-test scores being less than or equal to 0.05. Overall, more studies showed a statistically significant improvement in well being than studies where the improvement was not statistically significant. Although some studies did not achieve a statistically significant improvement in well-being, all showed a trend of improved well-being following the intervention. The graph below (Figure 2) shows the trends of QOLIE-31 scores before and after the intervention. Brandalise et al. (2019) scores were not included in this graph due to the scores being outside the accepted range for QOLIE-31 scoring.
Figure 2
Theme 2: Were there any similar characteristics
between studies that improved well-being?
The only common characteristics between the studies that improved well-being were that the participants were adults living with epilepsy who were exposed to behaviour therapy. There was a trend for well-being to improve in all the studies, with statistically significant improvements in 10 of the 16 studies (See Appendix 1). No common characteristics were found between studies deemed to have statistically significant results compared to those with statistically insignificant results. The type of behavioural intervention, the mode of delivery, the age and gender of participants, the type of facilitator and the duration of intervention did not appear to affect whether an intervention achieved statistically significant improvements in wellbeing.
Theme 3: Acceptability of the interventions
All of the studies in this review required the voluntary participation of people living with epilepsy, and that the participants be motivated to engage in the interventions, but very little feedback from participants was published. Qualitative data was included alongside quantitative data in Appendix 2. Of the seven studies which included qualitative data, five discussed positive user satisfaction. Leenen et al. (2018) received positive feedback from neurologists who reported that participants were better prepared for consultations and consultations were more effective. Pakpour et al. (2015) identified an improvement in the relationships between participants and their doctors. Participants in Hum et al’s (2019) study valued connecting with other people living with epilepsy. Hum et al. (2019) and Schroder et al. (2014) participants offered suggestions on how the interventions might be improved.
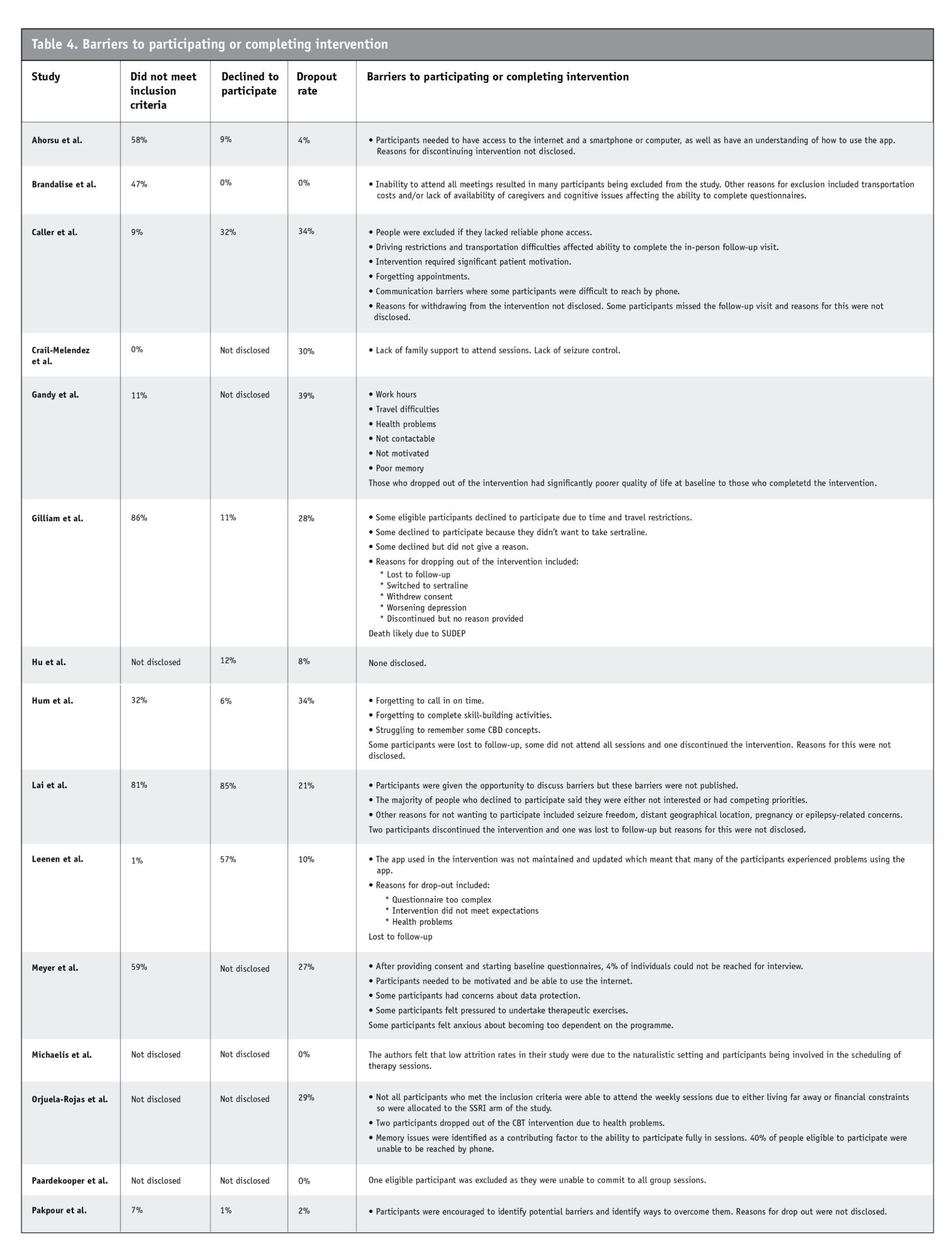
While most of the feedback was positive, Caller et al. (2016) and Leenen et al. (2018) participants struggled with the technology used in the interventions. Some participants in Meyer et al.’s (2018) study were concerned about data protection, felt pressured to undertake therapeutic exercises and were anxious about becoming too dependent on the intervention. Not all studies provided data on the number of people who did not meet inclusion criteria or who declined to participate. However, all studies provided data on drop-out rates. The number of people who did not meet exclusion criteria ranged from 0 per cent to 86 per cent, those who declined to participate ranged from 0 per cent to 85 per cent, and drop-out rates ranged from 0 per cent to 39 per cent. Only two studies identified barriers to participants enrolling and engaging fully with the interventions. Participation was negatively affected by transportation challenges, memory problems, poor internet/device literacy, low motivation, lack of support and health problems. The barriers that contributed to participating or completing the interventions are identified in Table 4.
DISCUSSION
Quantitative data analysis revealed a trend for improvement in well-being following participation in behavioural interventions. Feedback from participants, where available, was mostly favourable. Superficially, the qualitative and quantitative data appear to identify an improvement in well-being in people living with epilepsy following the use of behaviour therapy. This could imply that behaviour therapy is useful in improving the well-being of people living with epilepsy, but there are many limitations to consider.
It can be challenging to achieve robust, valid results in hard-to-reach populations such as those affected by stigma. McLaughlin et al. (2019) call these groups “hidden populations” and report that research results on participants recruited from these populations may differ from people of the same population who did not participate in the research. This makes it difficult to estimate the size of the population as well as to identify the characteristics and needs of the population (National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Division of Behavioural and Social Sciences and Education; Committee on National Statistics., 2018). Epilepsy is commonly associated with stigma, and the populations in the studies used for this review seem to reflect a similar phenomenon to McLaughlin’s “hidden populations”. In the studies where data on refusal to participate was included, there were high numbers of people living with epilepsy who declined to participate in the studies for various reasons. People with poorer well-being are less likely to participate and more likely to have less motivation. People with better well-being and who are more able to participate may not have as much room for improvement in well-being as people who are less able to participate.
Gandy et al. (2014) identified that participants with lower quality-of-life scores, particularly the cognitive function subscale, were more likely to drop out of the intervention, indicating that the intervention may be less suitable for people with cognitive difficulties. It may be that behavioural interventions are not desirable or practicable for many people living with epilepsy. It is recommended that attention is paid not only to the populations who are invited to and engage with the research, but also to those who are missing (Baumann & Cabassa, 2020). Many of the studies required people interested in participating in research to contact the authors to participate. In these studies, it can be assumed that disenfranchised and less motivated people would be harder to reach and, therefore, less likely to participate. The limited qualitative data in the studies may indicate that measurable, quantitative data was valued more highly than participation and feedback on the interventions. As well, this lack of qualitative information on people’s experience of living with epilepsy may increase the gap between what they value and desire and what is available to them.
While it seems that behaviour therapy improves well-being among some people living with epilepsy, it is important to consider other factors that may have improved well-being among the participants. Paardekooper et al. (2020) found that monitoring alone may act as a mediator for therapeutic change. Self-monitoring is a core component of behaviour therapy to identify where behaviour change is necessary (Psychology Tools, 2022). Completing the surveys and questionnaires required for participation in the studies may have contributed as mediators for change. Pakpour et al. (2015) had a multidisciplinary approach to the intervention whereby others involved in the participant’s care, including GPs, nurses and family members, also received a motivational interviewing intervention session. The improvement in the well-being of people living with epilepsy will likely have been affected by the health-care team and family members having a better understanding of epilepsy and management. Social interaction has a considerable effect on well-being (Szemere & Jokeit, 2014), and increased social interaction related to most of the interventions may have positively affected participants’ well-being.
Epilepsy affects slightly more males than females and is most prevalent in the 45 to 54-year age bracket. The mean ages of participants ranged from 28.69 to 49.3 years, and most were female. Epilepsy is more prevalent in lower socioeconomic groups, but it was not possible to identify the socioeconomic background of study participants from the available data. Ethnicity was also not identified in most of the studies, so it was impossible to determine if ethnic minorities were included. The exclusion of underserved populations is a common problem and creates “blind spots” in treatment and practice (Baumann & Cabassa, 2020). The studies in this review seem to have hefty “blind spots” due to the study populations varying considerably from general epilepsy populations. The difference between study population demographics and epilepsy population demographics also indicates “blind spots” and suggests that the study populations do not represent the general epilepsy population. This means that the results from the studies may not be transferable to the general epilepsy population. Also, these results indicate that
behaviour therapy improves well-being in only some people living with epilepsy.
This review has revealed how little is known about people living with epilepsy in New Zealand and how little is known about their needs. None of the studies were performed in New Zealand, so differences in health-care systems and cultures are likely. There is no data on the epidemiology or demographics of epilepsy in New Zealand, which makes it difficult to compare our epilepsy population with other populations. The absence of epilepsy demographics in New Zealand suggests that the impact of this relatively common condition is undervalued in this country. New Zealand’s “hidden population” of people living with epilepsy would be a challenging group to engage with, creating large gaps between people able and willing to participate in research and this disenfranchised population. This means that the information gathered from this review may not be able to be generalised to New Zealand’s epilepsy population.
RECOMMENDATIONS
The results of this review imply that behaviour therapy can improve well-being and that it is an acceptable intervention in some people living with epilepsy. To identify the usefulness of behaviour interventions in people living with epilepsy in New Zealand, further research is needed. The starting point of any future research is identifying the demographics of this population. The stigma associated with epilepsy and the isolation which commonly occurs as a result of this makes this a challenging group of people to reach, so considerable effort is required in gathering accurate data. New Zealand is currently incorporating SNOMED CT clinical terminology, which will be used in all areas of health (Ministry of Health, 2022). Once the demographics of epilepsy in New Zealand have been established, it would then be possible to identify the needs of people living with epilepsy as well as the needs of people working with this population.
This review has shown that behaviour therapy improves well-being in some people living with epilepsy but was unable to identify the needs of harder-to-reach people living with epilepsy. Building trust in this community would be necessary as it would be challenging to identify the demographics and needs of people who are “hidden”. There is no simple way to identify the needs of “hidden populations” but specialised sampling methods such as targeted sampling, time-location sampling, respondent-driven sampling and snowball sampling have been developed to target hard-to-reach populations. Education of health-care workers and the New Zealand public may help in raising awareness and reducing the stigma associated with epilepsy which may help reveal the needs of those living with epilepsy as well as those who care for them.
Further research into the needs of people living with epilepsy in New Zealand should be considered. Rather than investigate the effectiveness of behaviour therapies on the well-being of people living with epilepsy, research into what are the wants and needs of people living with epilepsy and those who care for them should be performed. Once these needs have been identified, feasibility studies should be performed to assess the effectiveness and practicality of any interventions. Specialised sampling methods would enhance participation. While quantitative data helps present data in a way that is meaningful for policymakers, qualitative data would be essential if wishing to identify data that is meaningful for people living with epilepsy, their whānau and health-care workers.
Any further research or plans to change practice should acknowledge the barriers to participation. Because transport was an issue that affected many study participants, it would be necessary to facilitate access to any interventions by using virtual and face-to-face delivery modes. Some participants struggled with technology, so appropriate support with any virtual interventions is essential. Memory and cognitive difficulties were also common problems and would need to be considered when creating any interventions or plans for further research. Many people living with epilepsy are socially isolated, and participants in these studies valued the opportunity to connect with other people living with epilepsy, so group interventions should be considered.
This review identifies that many people living with epilepsy have coexisting depression, memory concerns and poor motivation, yet these issues are rarely detected or acknowledged when managing epilepsy in New Zealand. These issues affect an individual’s ability to attend appointments, take appropriate treatment and participate in self-management. The well-being assessments identified in this review were useful in recognising overall concerns with well-being and some more specific areas such as physical, psychological and social well-being. It may be helpful to use similar assessment tools in everyday practice to place more of a focus on well-being, rather than epilepsy or “illbeing”. While this approach is unlikely to affect epilepsy management on a systemic level, it may lead to a better understanding of individual needs and improve an individual’s health-care experience.
LIMITATIONS
The limitations of the included studies are set out in Appendix 2. There are challenges in applying research findings conducted in other countries to the New Zealand context. Cultural differences are also likely present in the countries of origin, which may not be representative of the cultural diversity within their populations (Ahorsu et al., 2020; Gilliam et al., 2019; Lai et al., 2021; Leenan et al., 2018). The allocation of participants to interventions in some studies was not able to be blinded (Gilliam et al., 2019; Hu et al., 2020), and some studies had a small sample size (Hum et al., 2019; Michaelis et al., 2021; Orjuela-Rojas et al., 2015; Paardekoop et al., 2015) or a high participant dropout rate (Caller et al., 2016; Crail-Menendez et al., 2012; Gandy et al., 2014; Meyer et al., 2019). The interventions in some studies required internet access or visits to clinics which may have excluded some participants (Caller et al., 2016; Brandalise et al., 2019; Gandy et al., 2014; Orjuela-Rojas et al., 2015; Meyer et al., 2019).
CONCLUSION
This review identifies the characteristics of behavioural interventions that successfully improve the well-being of people living with epilepsy. Considerable effort is required to identify New Zealand’s epilepsy demographics and how to meet the needs of these people. This review has shown that behaviour therapy does improve well-being in some people living with epilepsy, but it is not possible to generalise these findings to New Zealand’s population. The participants of the studies in this review are a small sample of people living with epilepsy in countries with different health systems and different cultures. The first step in improving the well-being of people living with epilepsy in New Zealand is to identify who they are and how their condition burdens them, their whānau and the country. This will be a massive undertaking but will make it possible to identify the needs of this population and the health-care system. Only once this has been achieved can change be made at a systemic level.
ACKNOWLEDGEMENTS
The authors acknowledge the reviewers for their valuable feedback on earlier versions of this article.
REFERENCES
Ahorsu, D. K., Lin, C., Imani, V., Carlbring, P., Nygardh, A., Brostrom, A., Hamilton, K., & Pakpour, A. H. (2020). Testing an app-based intervention to improve insomnia in patients with epilepsy: A randomized controlled
trial. Epilepsy Behaviour, 112, 1-10.
Banks, J. (2021). ‘From the outside-in’ — Co-designing tools to promote independence and well-being in epilepsy care. International Journal of Integrated Care, 21(S1), 207.
Baumann, A. A., & Cabassa, L. J. (2020). Reframing implementation science to address inequities in healthcare delivery. BMC Health Services Research, 20, 1-9.
Blackwell, S. E., & Heidenreich, T. (2021). Cognitive behaviour therapy at the crossroads. International Journal of Cognitive Therapy, 14, 1-22.
Brandalise, M. H., de Araujo Filho, G. M., Centeno, R. S., Yacubian, E. M. T., & Jackowski, A. P. (2019). Effects of a brief psychotherapeutic intervention on resilience and behaviour in patients with drug-resistant mesial temporal lobe epilepsy and late seizure recurrence after surgery. Epilepsy Behaviour, 100, 106512.
Caller, T. A., Ferguson, R. J., Roth, R. M., Secore, K. L., Alexandre, F. P., Zhao, W., Tosteson, T. D., Henegan, P. L., Birney, K., & Jobst, B. (2016). A cognitive behavioural intervention (HOBSCOTCH) improves quality of life and attention in epilepsy. Epilepsy Behaviour, 51, 111-117.
Centers for Disease Control and Prevention. (2018). Well-being concepts.
Chan, R., Dear, B. F., Titov, N., Chow, J., & Suranyi, M. (2016). Examining internet-delivered cognitive behaviour therapy for patients with chronic kidney disease on haemodialysis: A feasibility open trial. Journal of Psychosomatic Research, 89, 78-84.
Crail-Meléndez, D., Herrera-Melo, A., Martínez-Juárez, I. E., & Ramírez-Bermúdez, J. (2012). Cognitive-behavioural therapy for depression in patients with temporal lobe epilepsy: A pilot study. Epilepsy Behaviour, 23(1), 52-56.
Cuijpers, P., van Straten, A., & Andersson, G. (2008). Internet-administered cognitive behaviour therapy for health problems: A systematic review. Journal of Behavioural Medicine, 31(2), 169-177.
Dewhurst, E., Novakova, B., & Reuber, M. (2015). A prospective service evaluation of acceptance and commitment therapy for patients with refractory epilepsy. Epilepsy & Behaviour, 46, 234-241.
Dwyer, P. A. (2020). Analysis and Synthesis. In C. E. Toronto & R. Remington, A step-by-step guide to conducting an integrative review (pp. 57–70). Springer.
Egan, S., Laidlaw, K., & Starkstein, S. (2015). Cognitive behaviour therapy for depression and anxiety in Parkinson’s disease. Journal of Parkinson’s Disease, 5(3), 443-451.
Fisher, R. S. (2014). A practical clinical definition of epilepsy. Epilepsia, 55(4), 475-485.
Gandy, M., Sharpe, L., Nicholson Perry, K., Thayer, Z., Miller, L., Boserio, J., & Mohamed, A. (2014). Cognitive behaviour therapy to improve mood inpeople with epilepsy: A randomised controlled trial. Cognitive Behaviour Therapy, 43(2), 153-166.
Gilliam, F. G., Black, K. J., Carter, J., Freedland, K. E., Sheline, Y. I., Tsai, W. Y., & Lustman, P. J. (2019). A trial of sertraline or cognitive behaviour therapy for depression in epilepsy. Annals of Neurology, 86(4), 552-560.
Grove, S. K., & Cipher, D. J. (2017). Statistics for nursing research: A workbook for evidence-based practice. Elsevier.
Harvey, M., & Land, L. (2022). Research methods for nurses and midwives. Sage.
Hofmann, S. G. (2021). The future of cognitive behavioural therapy. Cognitive Therapy & Research, 45, 383-384.
Hu, M., Zhang, C., Xiao, X., Guo, J., & Sun, H. (2020). Effect of intensive self-management education on seizure frequency and quality of life in epilepsy patients with prodromes or precipitating factors. Seizure, 78, 38-42.
Hum, K. M., Chan, C. J., Gane, J., Conway, L., McAndrews, M. P., & Smith, M. L. (2019). Do distance-delivery group interventions improve depressionin people with epilepsy? Epilepsy & Behaviour, 98, 153-160.
JBI. (2020). Critical appraisal tools.
Jones, F. J. S., Ezzeddine, F. L., Herman, S. T., Buchhalter, J., Fureman, B., & Moura, L. M. (2020). A feasibility assessment of functioning and quality-of-life patient-reported outcome measures in adult epilepsy clinics: A systematic review. Epilepsy Behaviour, 102, 106704.
Lai, S. T., Lim, K. S., Tang, V., & Low, W. Y. (2021). Mindfulness-based intervention to promote psychological well-being in people with epilepsy: A randomized controlled trial. Epilepsy & Behaviour, 118, 107916.
Leenen, L. A. M., Wijnen, B. F. M., Kessels, A. G. H., Chan, H., de Kinderen, R. J. A., Evers, S., van Heugten, C. M., & Majoie, M. (2018). Effectiveness of a multicomponent self-management intervention for adults with epilepsy (ZMILE study): A randomized controlled trial. Epilepsy Behaviour, 80, 259-265.
McLaughlin, K. R., Johnston, L. G., Gamble, L. J., Grigoryan, T., Papoyan, A., & Grigoryan, S. (2019). Population size estimations among hidden populations using respondent-driven sampling surveys: Case studies from Armenia. JMIR Public Health Surveillance, 5(1), e12034.
Meyer, B., Weiss, M., Holtkamp, M., Arnold, S., Brückner, K., Schröder, J., Scheibe, F., & Nestoriuc, Y. (2019). Effects of an epilepsy-specific internet intervention (Emyna) on depression: Results of the ENCODE randomized controlled trial. Epilepsia, 60(4), 656–668.
Michaelis, R., Schiepek, G., Heinen, G. M., Edelhäuser, F., & Viol, K. (2021). Process-oriented and personalized psychotherapeutic care for epilepsy:Interim results of a feasibility study. Epilepsy Behaviour, 124, 108313.
Ministry of Health. (2022). SNOMED CT.
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Division of Behavioral and Social Sciences and Education; Committee on National Statistics. (2018). Improving Health Research on Small Populations: Proceedings of aWorkshop.
Orjuela-Rojas, J. M., Martínez-Juárez, I. E., Ruiz-Chow, A., & Crail-Meléndez, D. (2015). Treatment of depression in patients with temporal lobe epilepsy: A pilot study of cognitive behavioural therapy vs. selective serotonin reuptake inhibitors. Epilepsy Behaviour, 51, 176-181.
Paardekooper, D., Thayer, Z., Miller, L., Nikpour, A., & Gascoigne, M. B. (2020). Group-based cognitive behavioural therapy program for improving poor sleep quality and quality of life in people with epilepsy: A pilot study. Epilepsy Behaviour, 104, 106884.
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., & Mulrow, C. D. (2021). The PRISMA 2020 statement: An updated guidelinefor reporting systematic reviews. BMJ, 372, n71.
Pakpour, A. H., Gholami, M., Esmaeili, R., Naghibi, S. A., Updegraff, J. A., Malloy, G. J., & Dombrowski, S. U. (2015). A randomized controlledmultimodal behavioural intervention trial for improving antiepileptic drugadherence. Epilepsy & Behaviour, 52, 133-142.
Peacock, J. L., & Peacock, P. J. (2011). Oxford handbook of medical statistics. Oxford University Press.
Programme on Mental Health World Health Organization. (1996). WHOQOLBREF introduction, administration, scoring and generic version of the assessment.
Psychology Tools. (2022). The CBT technique that’s overlooked, undervalued, and essential: Why is self-monitoring so important?
Schroder, J., Bruckner, K., Fischer, A., Lindenau, M., Kother, U., Vettorazzi, E.,
& Moritz, S. (2014). Efficacy of a psychological online intervention for depression in people with epilepsy: a randomized controlled trial. Epilepsia, 55(12), 2069-76.
Schroeder, K., Dumenci, L., Sarwer, D. B., Wheeler, D. C., & Hayat, M. J.(2022). Increasing quantitative literacy in nursing: A joint nursing-statistician perspective. Journal of Advanced Nursing, 78(4), e66–e68.
Spiegler, M. D. (2016). Contemporary behaviour therapy (6th ed.). Cengage Learning.
Szemere, E., & Jokeit, H. (2014). Quality of life is social — Towards an improvement of social abilities in patients with epilepsy. Seizure, 26, 12-21.
Toronto, C. E. (2020). Overview of the integrative review. In C. E. Toronto & R. Remington, A step-by-step guide to conducting an integrative review (pp. 1–9). Springer.
Vickrey, B. G., Perrine, K. R., Hays, R. D., Hermann, B. P., Cramer, J. A., Meador, K. J., & Devinsky, O. (1993). Quality of life in epilepsy QOLIE-31(version 1.0) scoring manual.

Daily doses – uncut news
| 30 Jul |
Backing our frontline rural health workforceRural communities across New Zealand will benefit from three new investments that will support the rural health workforce and help more people access care closer to home, Associate Health Minister Matt Doocey says. |
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


