
About the authors:Tara Malone, RN, MEd, NCATT, is a senior nursing lecturer at WITT – Te Pūkenga, Welbourn, Taranaki, New Zealand. She is also a clinical supervisor and trauma-informed coach. Helen Bingham, RN, MN, DipTertT, is a principal nursing lecturer at WITT – Te Pūkenga, Welbourne, Taranaki. She is a clinical supervisor and trauma-informed coach. This article was accepted for publication in March 2024. |
ABSTRACTAim: The aim of the study was to measure the effectiveness of an eight-week trauma-informed care credentialled course on the attitudes of health-care professionals towards being trauma-informed in their practice. Background: People engaged with mental health and addictions services are more likely to have experienced trauma than the general population. At the same time, health-care professionals working in these services are at risk of experiencing secondary or vicarious trauma as a result of working with people who have experienced trauma. Service providers need to ensure their workforce is equipped to recognise the multidimensional impact of traumatic experiences. Achieving this goal requires understanding service users’ experiences through a trauma-informed lens. Method: A quantitative quasi-experimental pre-and-post teaching study was undertaken, using purposive sampling. Data were collected pre- and post-course using the ARTIC-35, a reliable and validated tool. Results: Results indicate a significant difference in pre- and post-scores. Discussion: The findings suggest that participation in the course had positive outcomes for participants regarding their attitudes towards trauma-informed care. Conclusion: Trauma-informed care is considered best practice. Professional development in trauma-informed care for health-care professionals, including undergraduate and registered nurses (RNs), may improve care and outcomes across the health sector for those who have experienced trauma. Trauma-informed care not only benefits those receiving care, but also those delivering care by enhancing self-efficacy. As the largest professional health-care workforce, RNs are in a unique position to provide trauma-Informed care and influence the quality of care patients receive. |
||
KEYWORDShealth-care professionals, mental health and addictions, registered nurses, trauma-informed care, professional development |
|||


Introduction
THE NEED TO PROVIDE trauma-informed care across a range of social services is increasingly recognised because of the prevalence of trauma experiences (Baker et al., 2015; Isobel et al., 2021; Substance Abuse and Mental Health Services Administration [SAMHSA], 2014a; Sundborg, 2019). Such services include mental health and addictions, education, public health, criminal justice and social services (SAMHSA, 2014a; SAMHSA, 2014b; Ministry of Health [MOH], 2017). People who experience mental health and addiction challenges are more likely to have experienced trauma (Isobel, 2021; Muskett, 2014; SAMHSA, 2014a; Sweeney et al., 2018) which is often complex in nature (Cloitre et al., 2019). To provide trauma-informed care, health-care professionals need to understand and be responsive to the multidimensional impact of trauma on the person, their family/whānau and the wider community (Champine et al., 2018; MOH, 2017; Pihama & Smith, 2023).
Trauma-informed care is grounded in and directed by a thorough understanding of the neurological, biological, psychological and social effects of trauma and the prevalence of these experiences in persons who seek and receive mental health and addiction services (SAMHSA, 2014a). The importance of providing trauma-informed care is recognised internationally across health and social services (SAMHSA, 2014b; Niimura et al., 2019) because of its potential to help people with trauma experiences feel safe, heal from trauma and regain their personal developmental trajectories (SAMHSA, 2014b). Creating a more trauma-informed workforce, as well as maintaining that change, requires organisations to be interested in and committed to making the necessary changes to workplace culture (Yatchmenoff et al., 2017).
A trauma-informed workforce is one that assumes all those seeking care may have experiences of trauma; is aware the person seeking care risks being traumatised again by seeking care; and understands that care should be delivered using trauma-informed practices that are trauma-sensitive and minimise further harm (Royal Australian and New Zealand College of Psychiatrists [RANZCP], 2020). However the implementation of trauma-informed care across social services continues to be challenging (Berg-Poppe et al., 2022; Sundborg, 2019). One of the factors influencing the development a trauma-informed system is whether those working in the system have favourable attitudes towards trauma-informed care (Baker et al., 2015). Where attitudes are less favourable, interventions are needed to support attitudinal change.
Background
Conceptualising trauma can be challenging, as definitions and experiences of trauma are both extensive and narrow, as well as complex and diverse (McChesney, 2022). There are several definitions of trauma and trauma-informed care in the literature (Champine et al., 2022; Guest, 2020; Hopper et al., 2010; Pihama et al., 2020; SAMHSA, 2014a). For the purposes of this article, the predominantly Western world view from the United States Substance Abuse and Mental Health Services Administration (SAMHSA) will be used.
Trauma has been described as an event or series of events experienced by a person or persons that are perceived as physically, or emotionally harmful, or life threatening, which has lasting adverse effects on the individual’s ability to function mentally, physically, socially, emotionally and spiritually (SAMHSA, 2014b). This includes, but is not limited to: trauma that occurs as a single event to a single person (SAMHSA, 2014b); in communities, such as the immediate experiences of terrorism; or intergenerationally, such as the experience of colonisation in Aotearoa, New Zealand (Fortuna et al. 2022); or vicariously, through hearing about or witnessing another’s experience (SAMHSA, 2014b). Experiences of trauma are not uncommon, with the World Health Organization gauging that approximately 70 per cent of people will experience a traumatic event in their lifetime (Kessler, 2017).
It is essential to understand the particular impact of developmental trauma and adverse childhood experiences (ACEs) — studies report the affect of such events on brain architecture in the first 1000 days from conception is critical (Felitti et al., 1998; Hambrick et al., 2019; Linnér & Almgren, 2020; Woo Baidal et al., 2016). Influential factors such as environment, genetics, epigenetics and social determinants profoundly affect brain development (Hambrick et al. 2019). Brain development is over-sensitised by prolonged activation of the stress response (Avery et al. 2020), sensitising future neural responses to even minor occasions of perceived stress (Van der Kolk, 2005). It is important to expand the definition of ACEs to include experiences outside the home to ensure that solutions include macro community and society-focused interventions, rather than only that of the individual or family/whānau (Metzler, 2017). Expanded ACEs include experiences such as poverty, discrimination, bullying and community violence caused by structural racism, and structural violence often experienced by minority populations (Bernard et al., 2021). The 10 ACEs originally described by Felitti et al. (1998) are displayed in Table 1.
Table 1. The 10 ACEs originally identified by Felitti et al. (1998)
| Abuse | Neglect | Household dysfunction |
| 1 Physical 2 Emotional 3 Sexual |
4 Physical 5 Emotional |
6 Mental illness 7 Violence towards mother 8 Divorce 9 Substance abuse 10 Incarcerated family member |
Since the original ACE study undertaken by Felitti et al. (1998), there has been a growing consensus that ACEs increase the risk of an individual experiencing mental health and addiction issues later in life, as well as the likelihood of involvement with the criminal justice system (Moffitt et al., 2013; Skarupski et al., 2016). Trauma experiences correlate negatively with mental, physical and social wellbeing (Siegel, 2012), resulting in costly public health problems (Isobel & Edwards, 2017), health inequality, poorer long-term health outcomes and reduced quality of life (Reid et al., 2023). Services need to be equipped to improve users’ experience of them, as well as the experiences of those working in them. A service practising trauma-informed care can be enabled by developing a workforce which asks: “What has happened to you?” rather than “What is wrong with you?” (Sweeney et al. 2018)
In contemporary society, events such as ongoing intergenerational and historical trauma (Smallwood et al., 2021), natural disasters (Fergusson et al., 2015) and the global trauma of the COVID-19 pandemic (Masiero et al., 2020) have further perpetuated or exposed people to mass trauma experiences. Recent literature suggests that the impact of the global mass trauma experienced from COVID-19 has resulted in a second “trauma” pandemic, occurring due to the distress and psychological harm caused by the original pandemic (Goddard et al., 2021). Addressing historical and intergenerational trauma is a priority for services in countries where the colonisation of the indigenous people (for example Aotearoa, New Zealand) has occurred (Darwin et al., 2023; McClintock et al., 2018; Patterson et al., 2018). The ongoing effects of the trauma experienced through loss of land, forceable removal of children and acculturation are seen internationally among indigenous communities such as Māori, Aboriginal and Torres Strait Islanders and Canadian First Nations peoples (Menzies, 2019). In Aotearoa New Zealand, for instance, nearly two-thirds of adults who identify as Māori have experienced one or more traumatic events, compared to half of adults in the general population (Hirini et al., 2005). Statistically, Māori continue to be over-represented across health and trauma-based statistics due to the impacts of ongoing historical, intergenerational, situational and cumulative trauma (McClintock et al., 2018). The benefits of a trauma-informed approach to care for those receiving and delivering services are widely recognised and supported in the literature (Morrissey et al. 2005; Mental Health Coordinating Council, 2018; Sweeney et al., 2016), but this care must be carried out in a culturally appropriate way (Pihama et al., 2020; Pihama & Smith, 2023; Wirihana & Smith, 2014).
There are two important requirements for the provision of trauma-informed care: firstly, the delivery of care must be sensitive to a person’s experiences of trauma; secondly, iatrogenic trauma should not occur while the person is receiving care (Isobel, 2021; Pfeiffer & Grabbe, 2022). Iatrogenic trauma refers to the trauma or re-traumatisation which can be experienced by a person in the process of seeking care, where their behaviours are viewed as symptoms of illness (What is wrong with you?), rather than as coping adaptations to trauma experiences (What has happened to you?) (Sweeney et al., 2018). Non-trauma-informed responses to such behaviours may result in power imbalances, intrusive procedures, insensitive or humiliating interactions (Pfeiffer & Grabbe, 2022), coercive practices such as forced medication or restraint (Gooding et al., 2020), and culturally unsafe care (Pihama et al., 2017).
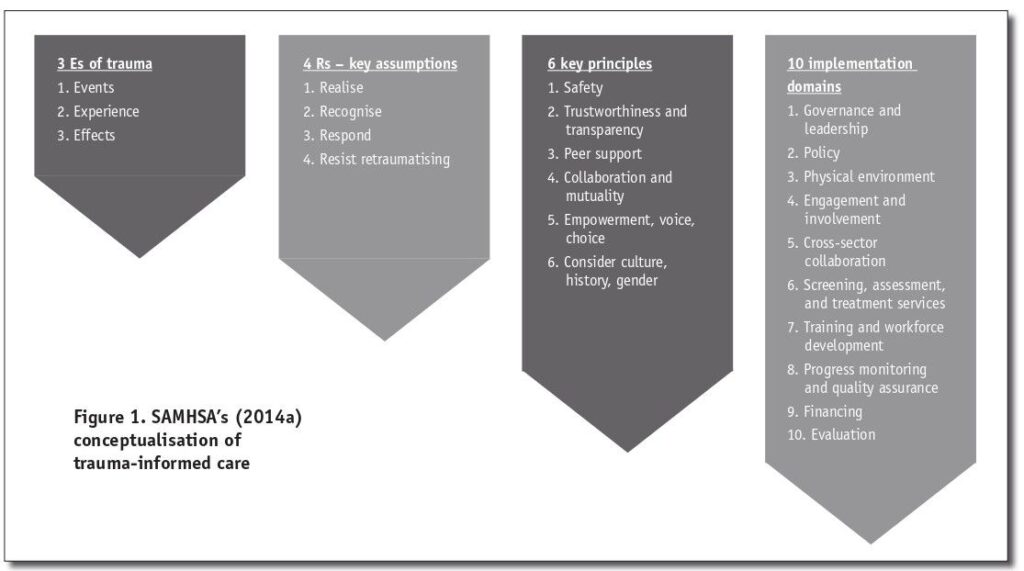
The principles of trauma-informed care focus on the individual’s strengths and competencies, and require those delivering care to work compassionately and responsively to ensure safety, promote integrity, and support and empower people who have experienced trauma. A strengths-based service creates opportunities for those seeking care to rebuild a sense of control and empowerment (SAMHSA, 2014a: Te Rau Ora et al., 2021). Figure 1 displays SAMHSA’s (2014a) concept of trauma-informed care.
Without an understanding of the principles of trauma-informed care, professionals may feel that they are not equipped to support those who have experienced trauma, often perceiving listening to a trauma narrative as being outside their scope of practice (Palfrey et al., 2018). It is also important to note that hearing a trauma narrative may not actually be helpful to the person telling their story, as re-traumatisation may occur for the narrator at each retelling (Sweeney et al., 2018). Implementing trauma-informed principles across all domains of a service aims to reduce this risk (SAMHSA, 2014b). There is also the potential risk of harm from vicarious trauma for the listener (Devilly et al., 2009). The very nature of professions such as nursing places nurses at a high risk of vicarious trauma through clinical exposure (Pfeiffer & Grabbe, 2022).
Vicarious trauma was originally coined by McCann and Pearlman (1990) as a specific and limited term to describe the unique, adverse, and accumulative changes that can occur to health-care professionals who engage in an empathetic relationship with those they care for. This places the health-care professional in a difficult position as trauma-informed care requires them to provide care that is empathic. Empathic engagement, however, has been associated with vicarious trauma (Gerace, 2018), specifically through the sharing of often detailed and graphic narratives during therapeutic engagement (Branson, 2019). Vicarious trauma may result in the health-care professional experiencing diminished emotional states, symptoms of traumatic stress or even re-traumatisation (Pfeiffer & Grabbe, 2022).
The present study
The course
This study explores the effectiveness of an eight-week trauma-informed care course on the attitudes of health-care professionals, including RNs, towards the use of trauma-informed care in their practice. The course was developed by two nurse lecturers employed at an Aotearoa, New Zealand polytechnic (the study site) and was approved by the relevant qualifications authority as a level 7, 15-credit micro-credential. The course aims to develop the proficiency of those working in health care in the principles, knowledge and practice of trauma-informed care, when caring for people with multidimensional experiences of trauma. The course learning outcomes are displayed in Table 2.
Table 2. Course learning outcomes
| No. | Learning outcome |
| 1 | Critically analyse the widespread impact of multidimensional trauma on the person holistically. |
| 2 | Use a range of indepth sciences to inform clinical judgments and decision-making using a trauma-informed approach. |
| 3 | Critically examine and reflect on own practice and knowledge using trauma-informed principles to deliver care of self and others. |
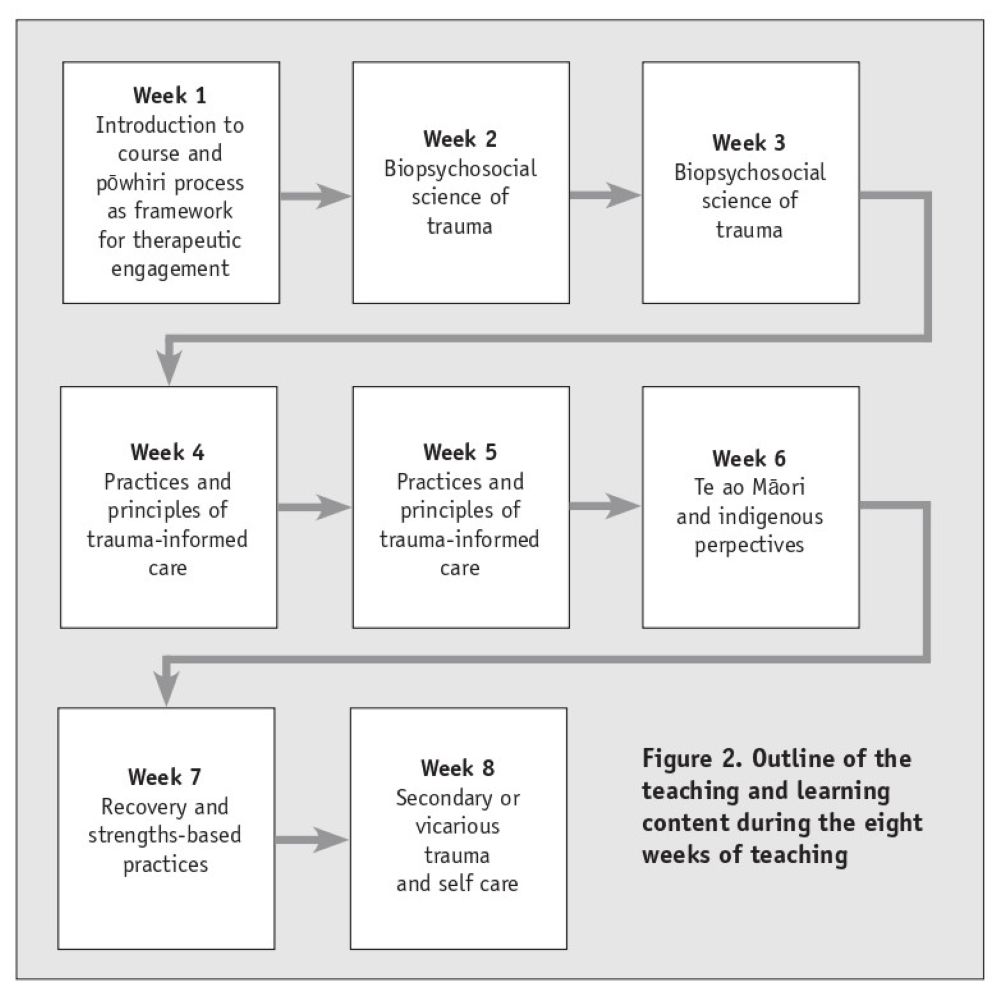
The course was developed as a hybrid learning experience, which comprised 150 hours of learning. Week one and week eight included an eight-hour face-to-face workshop. Learning was delivered asynchronously, online, over a period of eight weeks (see Figure 2). This style of learning was chosen to meet the needs of those who are currently in employment. Teaching and learning material drew on work undertaken by SAMHSA, along with a wide range of evidence-based material, both national and international, to enable participants to meet the course learning outcomes. There were four assessments, with participants required to gain a 50 per cent pass rate to gain this formal qualification.
Methods
Study design and participants
This study used an exploratory, quantitative quasi-experimental pretest-posttest design. Convenience sampling (Cohen et al., 2017) was used to recruit participants. Twenty-seven participants on the course volunteered to participate in the research. An information sheet outlining the research and inviting participation was distributed to all enrollees. Participants were from a broad and diverse demographic, including age, gender, profession, years in profession and ethnicity.
Data collection and instruments
Data were collected pre- and post-course, using the Attitudes Related to Trauma-Informed Care-35 (ARTIC) scale (Baker et al. 2015). The ARTIC-35 is designed to be used in settings that have not yet begun implementation of trauma-informed care and has previously shown good internal consistency, at 0.91, and good test–retest reliability, at 0.75 (Niimura et al., 2019). The ARTIC-35 is a 35-item self-report scale which uses a bipolar seven-point Likert scale to measure the participants’ personal attitudes, with higher scores indicating a more favourable attitude. An example of a more favourable attitude, in the context of this study, is: “Clients’ learning and behaviour problems are rooted in their history of difficult life events”, whereas the less favourable attitude is: “Clients’ learning and behaviour problems are rooted in their behavioural or mental health conditions.” Attitudes are measured across five sub-scales in relation to the participant’s current work (see Table 3). The instrument is scored by inputting the exact responses of the participants into a predetermined ARTIC scoring Excel spreadsheet (Baker et al., 2015). STROBE guidelines for reporting were followed when reporting this study.
Table 3. The five ARTIC sub-scales and an explanation of each attitude
| 1 | Underlying causes of problem behaviour and symptoms. Behaviour and symptoms are adaptations and malleable, as oppposed to being intentional and fixed. |
| 2 | Responses to problem behaviour and symptoms. Emphasises relationships, kindness, flexibility and safety as agents of behaviour and symptom change as opposed to rules, consequences and accountability. |
| 3 | On-the-job behaviour. This endorses empathy-focused staff behaviour as opposed to control-focused staff behaviour. |
| 4 | Self-efficacy at work: Endorses feeling able to meet the demands of working with traumatised people, as opposed to feeling unable to meet the demands. |
| 5 | Reactions to work. This endorses appreciating the effects of secondary trauma and vicarious traumatisation, as opposed to coping by ignoring or hiding the impact. |
Ethics
Ethical approval to undertake the study was granted by the research study site (20/TLC09/06). The participants signed informed consent forms when agreeing to participate in the study and were advised they could leave the study at any stage as participation was voluntary. The researchers acknowledge an existing professional relationship with some of the participants who voluntarily took part in the study. Opportunity to participate in the study was invited by a third party. Data were collected anonymously to protect the identity of the participants.
Analysis
Participant characteristics were summarised and included gender, age and, for the nurses involved, years in the nursing profession. Participants’ data were entered directly into an ARTIC Excel scoring tool which calculated overall results, including those for each of the five sub-scales. The same process was followed for the data sets which were collected at pre-training (P1) and immediately post-training (P2). Standard deviations (SD) for each data collection point were obtained and confidence intervals (CI) for the average scores between time points were estimated. Scores were calculated to 3 significant figures (3sf). The t-test was used for each data set.
Results
Participant characteristics
A total of 27 participants took part in this study, with data collected for all 27 at P1, and for 24 at P2. All 27 participants successfully completed the course. Participant demographic characteristics are displayed in Table 4 (below). The study participants consisted of 66 per cent RNs (n=18) from mental health and addiction services, but also included participants from social services, drug and alcohol services, psychological services and Corrections. Ages ranged from 25 to 64 years; three identified as male and 24 as female. The average years employed in mental health and addiction services were calculated as 18.
Table 4. Participant demographics
| Characteristics | n | |
|---|---|---|
| Gender | Male | 3 |
| Female | 24 | |
| Age groups | 18-24 | 0 |
| 25-34 | 2 | |
| 35-44 | 5 | |
| 45-54 | 13 | |
| 55-64 | 7 | |
| 65+ | 0 | |
| Mean years in profession | 18 | |
| Number of registered nurses | 18 | |
| Total participants | 27 | |
Effectiveness of the course
Table 5 represents the average scores for the ARTIC instrument at each of the two data collection points, the number of respondents and the standard deviation between scores. The scores for each of the five subscales are shown in Table 6 and represent data collection during pre-training (P1) and immediately post-training (P2). Scores for each subscale were calculated by summing up the items within the subscale. Items for each subscale are written to characterise an attitude favourable to trauma-informed care, and are then paired with the opposite attitude. The scores indicate that participants increased their favourable attitudes to trauma-informed care across all five subscales during the teaching phase (Table 6). A change in scale scores between data collection P1 and P2 is noted (Table 7), with the confidence interval (CI) for difference in mean scores (0.098, 0.789) at p = .013. The average score increased by 0.444 between these time periods. The CI and p-value provide evidence against the null hypothesis, indicating that the observed increase in the average score was statistically significant.
Table 5. No of respondents, average scores and SD between scores
| Point 1 Pre-training |
Point 2 Post-training |
|
|---|---|---|
| n | 28 | 24 |
| Average score | 5.46 | 5.90 |
| SD | 0.64 | 0.59 |
Table 6. ARTIC sub-scale scores at each of the data collection points, and SD
| Data collection point |
Underlying causes of problem behaviour and symptoms |
Responses to problem behaviour and symptoms |
On-the-job behaviour |
Self-efficacy at work |
Reactions to work |
n= | Total | SD |
| P1 | 5.44 | 5.72 | 5.67 | 5.07 | 5.40 | 28.00 | 5.46 | 0.64 |
| P2 | 6.05 | 6.38 | 6.25 | 5.10 | 5.74 | 24.00 | 5.90 | 0.58 |
Table 7. Mean change, confidence interval, p-value and statistical difference between data collection points
| Data collection points |
Mean change | Lower CI limit | Upper CI limit | p-value | Significance |
| P1 v P2 | 0.443 | 0.097 | 0.789 | .013 | sig* |
Discussion
This study evaluated the effectiveness of an eight-week credentialled course on the attitudes of health professionals towards using a trauma-informed approach to care. The findings suggested that participation in the course resulted in positive attitudinal change in those working in the mental health sector, towards using a trauma-informed care approach. A review of the literature revealed that to the best of our knowledge this is the first study of its kind in Australasia.
Participants completed the online course as part of their professional development. Significant changes in attitude towards trauma-informed care between P1 (pre-training) and P2 (immediately post-training) indicated that the change mostly occurred during the teaching and learning phase of the study. This finding is consistent with other studies (Lotzin et al., 2018; Niimura et al., 2019; Palfray et al., 2018) and proposes that attitudinal change was transferred to the workplace setting, with course participants showing more sensitivity to those who have experienced trauma.
The increase in favourable attitudes towards trauma-informed care for subcategories “underlying causes of problem behaviour and symptoms” and “responses to problem behaviour and symptoms” suggests that participants were able to use the knowledge learned in the course in their work. They were able to use this new knowledge to underpin how they interpreted and responded to the behaviours of those who had experienced trauma, shifting from asking “What is wrong with you?” to “What has happened to you?”
Stokes et al. (2017) purport that it is essential for staff to understand the impact of trauma in order to provide supportive strategies to manage the impact of trauma experiences. Providing a supportive and safe environment demonstrates the trauma-informed principles of safety, trustworthiness, collaboration, empowerment and choice (SAMHSA, 2014b), thereby reducing the risk of re-traumatisation for the person receiving care.
Providing care that encompasses the core principles of trauma-informed care reduces the risk of a “power over” relationship between the health-care professional and person seeking care (SAMHSA, 2014; Sweeney et al., 2018) and may therefore reduce re-traumatisation. Favourable results for these two subcategories, as well as “on the job behaviour”, also suggest that the participants may have considered opting for less restrictive practices, such as sensory modulation, rather than traditional restrictive practices, such as seclusion, when providing care (Meredith et al., 2018). A health-care professional who asks the person about their sensory preferences and sensory needs during trauma-informed assessment and care planning, is supporting the person’s self-regulation, which results in a collaborative and mutual approach to care (Brown & Knowles, 2021). Additional investigation is warranted to further test this hypothesis.
An increase in favourable attitudes between P1 and P2 for subcategories “on the job behaviour”, “self-efficacy at work” and “reactions to work” suggests that putting the learning into practice helped to further embed a change in attitude for the participants. Having the confidence to undertake a task correlates with successful completion of the task (Bandura, 1977) which enhances self-efficacy. Self-efficacy has been defined as believing in one’s capability to succeed when faced with unique situations and activities (Berg-Poppe, 2022). The use of education (Hough et al., 2019; Kerig, 2019; Sweeney et al., 2016) and personal and vicarious experiences (Gavriel, 2016) as a means of developing self-efficacy is well-supported in the literature. If the workforce holds positive attitudes and beliefs towards their ability to implement trauma-informed care principles and practices, there is a higher likelihood of successful implementation (Berg-Poppe, 2021). Health-care professionals must recognise their workforce’s personal experiences when supporting trauma survivors. This acknowledgment helps prevent vicarious trauma, burnout, job dissatisfaction and high attrition rates (Isobel & Thomas, 2022; Slayter et al., 2018).
A previous study by Kerns et al. (2016) suggests positive shifts in attitudes towards trauma-informed care are higher among those who have less experience in the workforce, as opposed to those with longer experience. In the current study, positive changes in attitude were identified despite the mean years of professional practice among participants being 18 years.
Consideration of when trauma-informed knowledge should be introduced to the workforce is important. Pfeiffer and Grabbe (2022) propose that incorporating trauma-informed care into undergraduate nursing curricula may develop undergraduates’ self-knowledge, helping them to identify strategies for self-care and to build their resilience, thus enhancing their ability to work with those who have trauma experiences. New graduates would enter the workforce with some knowledge and skills of the practice, their self-efficacy enhanced through education (Hough et al., 2019; Kerig, 2019; Sweeney et al., 2016) and providing a protective factor against vicarious trauma (Zhang et al., 2022). Goddard et al. (2021) believe teaching these skills at undergraduate level is imperative, given the global impact of the trauma associated with COVID-19 on the health-care workforce (Choi et al., 2020). A systematic review undertaken by Nizum et al. (2020) highlights the benefits of all RNs undergoing professional development training in trauma-informed care to ensure a common understanding and approach to the provision of trauma-informed services.
One of the barriers to implementing trauma-informed care is workplace culture (Happel & Harrow, 2010). Workplace culture has been defined by Long and Helms Mills (2010) as the types of attitudes and ways of working shared by employees of an organisation, including how employees value their work, support each other and feel supported by their organisation. A study by Isobel et al. (2021) highlighted the need for organisational leadership that is accountable, and provides direction and commitment to implementing trauma-informed practices and principles. These findings are further supported in a literature review undertaken by Huo et al. (2023). Although our study showed significant positive change in participants’ attitudes, there is scope for additional investigation into the role organisational leadership has in supporting trauma-informed practices in the workplace.
Limitations
The sample size was small, which limits the generalisability of the results. Using a paired t-test during analysis would have added further rigour to the study. A mixed-methods approach could have allowed for the collection of rich qualitative data, enabling a deeper understanding of the phenomena. Future iterations of this study will consider using a mixed-methods approach.
This research was conducted using predominantly Western world views of trauma and trauma-informed practices and principles. Future versions of the study should include needs, preferences and approaches to trauma and trauma-informed care from a te ao Māori perspective, with a particular focus on Māori practices of healing. The use of mātauranga Māori and tikanga practices are acknowledged as essential to reduce the risk of iatrogenic traumatisation from culturally unsafe care.
Conclusion
This study addresses a gap in the literature and reports on the significant changes in attitudes experienced by participants in an eight-week course on trauma-informed care, designed to help them incorporate it into their professional practice. Becoming trauma-informed is not a “ticking off a list of actions” style of learning. To be trauma-informed requires a shift in the thinking, attitude, behaviour and ideology that underpins the health professional’s approach to care. For the introduction of trauma-informed care to be truly successful in a health service, there need to be system-wide trauma-informed policies, procedures and practices. The positive findings of this study show how heath providers can meet expectations that their services be trauma-informed and how trauma-informed care might be embedded across all health and social services.
Relevance for clinical practice
Staff acquiring knowledge about the neurobiological effects of trauma experiences is imperative as the first step towards developing a trauma-informed workforce (Isobel et al., 2021; Sweeney et al., 2018). The positive outcomes of this study suggest that the micro-credential course used here could be delivered both locally and nationally, and that training in trauma-informed care should be made mandatory across all health-care setting and beyond.
Trauma-informed care is considered best practice (SAMHSA, 2014a, b). This is supported by Aotearoa, New Zealand national organisations such as Te Pou (2018) (New Zealand’s workforce development centre for mental health, addictions and disability staff), and the recommendations of government reports on the provision of care in the mental health and addictions sector (Patterson et al., 2018). To the best of our knowledge, there is currently no national approach to embedding this knowledge into practice in Aotearoa, New Zealand.
We recommend implementing mandatory trauma-informed care training as part of national nursing workforce professional development, as well as embedding this knowledge throughout nursing curricula.
Using education to develop a trauma-informed workforce not only benefits those receiving care, but also those delivering care by enhancing self-efficacy. Through the provision of care underpinned by the six key principles of trauma-informed care (SAMHSA, 2014a), a health-care workforce will ask people they care for “What has happened to you?” rather than “What is wrong with you?” As the largest professional health-care workforce, providing care across all health-care contexts to patients across the lifespan, RNs are in a unique position to provide trauma-informed care and influence the quality of care patients receive (Fleishman et al., 2019). Trauma-informed care must also include culturally appropriate practices when caring for Māori. It is imperative that trauma-informed care acknowledges trauma and healing as it is understood from a te ao Māori perspective, due to ongoing trauma and marginalisation associated with colonisation (Pihama et al., 2020; Pihama & Smith, 2023).
ACKNOWLEDGEMENTS
We would like to acknowledge WITT – Te Pūkenga for the professional development support to complete this study, and Dr Janine Wright who assisted with data input and provided statistical expertise during data analysis.
We would like to acknowledge Tuari Rewiti (Ngāti Maniapoto, Raukawa, Ngā Rauru Kītahi), kaitakawaenga at WITT – Te Pūkenga, for providing guidance about using a cultural framework for engagement during the face-to-face workshops.
We would also like to acknowledge all who have a lived experience of trauma and hope that the positive outcomes of this study reinforce the need for health professionals to be trauma-informed when caring for those with experiences of trauma.
Statements
Authorship: All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and all authors agree with the manuscript.
The authors confirm contribution to the paper as follows:
Study conception and design: Malone, Bingham.
Data collection: Bingham.
Analysis and interpretation of results: Malone.
Draft manuscript preparation: Malone, Bingham.
Both authors reviewed the results and approved the final version of the manuscript.
Funding: The authors received no specific research grant or funding to complete the study. Funding for the purchase of the ARTIC tool used to collect data was received from WITT – Te Pūkenga.
Conflict of interest: The researchers acknowledge an existing professional relationship with some of the participants who voluntarily took part in the study. Opportunity to participate in the study was invited by a third party. Data were collected anonymously to protect the identity of the participants.
References
Avery, M., H., Galvin, E., Misso, M., Savaglio, M., & Skouteris, H. (2020). Systematic review of school-wide trauma-informed approaches. Journal of Child & Adolescent Trauma, 14(3), 381-397.
Baker, C. N., Brown, S. M., Wilcox, P. D., Overstreet, S., & Arora, P. (2015). Development and psychometric evaluation of the Attitudes Related to Trauma-Informed Care (ARTIC) Scale. School Mental Health, 8(1), 61-76.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191-215.
Berg-Poppe, P., Anis Abdellatif, M., Cerny, S., LaPlante, K., Merrigan, M., & Wesner, C. (2022). Changes in knowledge, beliefs, self-efficacy, and affective commitment to change following trauma-informed care education for pediatric service providers. Psychological Trauma, 14(4), 535-544.
Bernard, D. L., Calhoun, C. D., Banks, D. E., Halliday, C. A., Hughes-Halbert, C., & Danielson, C. K. (2021). Making the “C-ACE” for a Culturally-Informed Adverse Childhood Experiences Framework to understand the pervasive mental health impact of racism on black youth. Journal of Child and Adolescent Trauma, 14, 233-247.
Branson, D. C. (2019). Vicarious trauma, themes in research, and terminology: A review of literature. Traumatology, 25(1), 2-10.
Brown, C., & Knowles, R. L. (2021). Sensory processing preferences for people recovering from addictions. American Journal of Occupational Therapy, 75(S2), 7512500001p1.
Champine, R., Matlin, S., Strambler, M., & Tebes, J. (2018) Trauma-informed family practices: Toward integrated and evidenced-based approaches. Journal of Child and Family Studies, 27, 2732-2734.
Champine, R., Hoffman, E., Matlin, S., Strambler, M. J., & Tebes, J. K. (2022). “What does it mean to be trauma-informed?”: A mixed-methods study of a trauma-informed community initiative. Journal of Child and Family Studies, 31, 459-472.
Choi, K. R., Heilemann, M. V., Fauer, A., & Mead, M. (2020). A second pandemic: Mental health spillover from the Novel Coronavirus (COVID-19). Journal of the American Psychiatric Nurses Association, 26(4), 340-343.
Cloitre, M., Hyland, P., Bisson, J. I., Brewin, C. R., Roberts, N. P., Karatzias, T., & Shevlin, M. (2019). ICD‐11 Posttraumatic stress disorder and Complex posttraumatic stress disorder in the United States: A population‐based study. Journal of Traumatic Stress, 32(6), 833-842.
Cohen, L., Manion, L., & Morrison, K. (2017). Research methods in education. Taylor & Francis.
Darwin, L., Vervoort, S., Vollert, E., & Blustein, S. (2023). Intergenerational trauma and mental health. Catalogue number IMH 18, Australian Institute of Health and Welfare, Australian Government.
Devilly, G. J., Wright, R., & Varker, T. (2009). Vicarious trauma, secondary traumatic stress or simply burnout? Effect of trauma therapy on mental health professionals. Australian & New Zealand Journal of Psychiatry, 43(4), 373-385.
Fergusson, D. M., Boden, J. M., Horwood, L. J., & Mulder, R. T. (2015). Perceptions of distress and positive consequences following exposure to a major disaster amongst a well-studied cohort. Australian & New Zealand Journal of Psychiatry, 49(4), 351-359.
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245-258.
Fleishman, J., Kamsky, H., & Sundborg, S. (2019). Trauma-informed nursing practice. Online Journal of Issues in Nursing, 24(2), 1-9.
Fortuna, L. R., Tobón, A. L., Anglero, Y. L., Postlethwaite, A., Porche, M. V., & Rothe, E. M. (2022). Focusing on racial, historical and intergenerational trauma, and resilience: A paradigm to better serving children and families. Child and Adolescent Psychiatric Clinics of North America, 31(2), 237-250.
Gavriel, J. (2016). Perceived self-efficacy. Education for Primary Care, 27(2), 144-145.
Gerace, A., Oster, C., O’Kane, D., Hayman, C. L. & Muir-Cochrane, E. (2018). Empathic processes during nurse-consumer conflict situations in psychiatric inpatient units: A qualitative study. International Journal of Mental Health Nursing, 27(1), 92-105.
Goddard, A., Jones, R. W., Esposito, D., & Janicek, E. (2021). Trauma informed education in nursing: A call for action. Nurse Education Today, 101, 104880–104880.
Gooding, P., McSherry, B., & Roper, C. (2020). Preventing and reducing ‘coercion’ in mental health services: An international scoping review of English-language studies. Acta Psychiatrica Scandinavica, 142(1), 27-39.
Guest, H. (2021). A concept analysis of trauma‐informed care. Nursing Forum, 56(4), 1000-1007.
Hambrick, Brawner, T. W., Perry, B. D., Brandt, K., Hofmeister, C., & Collins, J. O. (2019). Beyond the ACE score: Examining relationships between timing of developmental adversity, relational health and developmental outcomes in children. Archives of Psychiatric Nursing, 33(3), 238-247.
Happell, B., & Harrow, A. (2010). Nurses’ attitudes to the use of seclusion: A review of the literature. International Journal of Mental Health Nursing, 19, 162-168.
Hirini, P., Flett, R., Long, N., & Millar, M. (2005). Frequency of traumatic events, physical and psychological health among Maori. New Zealand Journal of Psychology, 34(1) 20-27.
Hopper, E. K., Bassuk, E. L., & Olivet J. (2010). Shelter from the storm: Trauma-informed care in homelessness services settings. Open Health Services and Policy Journal, 3, 80-100.
Hough, J., Levan, D., Steele, M., Kelly, K., & Dalton, M. (2019). Simulation-based education improves student self-efficacy in physiotherapy assessment and management of paediatric patients. BMC Medical Education, 19(1), Article 463.
Huo, Y., Couzner, L., Windsor, T., Laver, K., Dissanayaka, N. N., & Cations, M. (2023). Barriers and enablers for the implementation of trauma-informed care in healthcare settings: a systematic review. Implementation Science Communications, 4(1), 49-49.
Isobel, S., & Edwards, C. (2017). Using trauma informed care as a nursing model of care in an acute inpatient mental health unit: A practice development process. International Journal of Mental Health Nursing, 26(1), 88-94.
Isobel, S. (2021). The ‘trauma’ of trauma-informed care. Australasian Psychiatry, 29(6), 604-606.
Isobel, S., Wilson, A., Gill, K., Schelling, K., & Howe, D. (2021). What is needed for Trauma Informed Mental Health Services in Australia? Perspectives of clinicians and managers. International Journal of Mental Health Nursing, 30(1), 72-82.
Isobel, S., & Thomas, M. (2022). Vicarious trauma and nursing: An integrative review. International Journal of Mental Health Nursing, 31(2), 247-259.
Kerig, P. K. (2019). Enhancing resilience among providers of trauma-informed care: A curriculum for protection against secondary traumatic stress among non-mental health professionals. Journal of Aggression, Maltreatment & Trauma, 28(5), 613-630.
Kerns, S., Pullmann, M., & Negrete, T. (2016). Development and implementation of a child welfare workforce strategy to build a trauma informed system of support for foster care. Child Maltreatment, 21, 135-146.
Kessler, R. C., Aguilar-Gaxiola, S., Alonso, J., Benjet, C., Bromet, E. J., Cardoso, G., Degenhardt, L., de Girolamo, G., Dinolova, R. V., Ferry, F., Florescu, S., Gureje, O., Haro, J. M., Huang, Y., Karam, E. J., Kawakami, M., Lee, S., Lepine, J.-P., Levinson, D., … Koenen, K. C. (2017). Trauma and PTSD in the WHO World Mental Health Surveys. European Journal of Psychotraumatology, 8(sup5), 1353383.
Linnér, A., & Almgren, M. (2020). Epigenetic programming – The important first 1000 days. Acta Paediatrica, 109(3), 443-452.
Long, B. S., & Helms Mills, J. (2010). Workplace spirituality, contested meaning, and the culture of organization: A critical sensemaking account. Journal of Organizational Change Management, 23(3), 325-341.
Lotzin, A., Buth, S., Sehner, S., Hiller, P., Martens, M.-S., Pawils, S., Metzner, F., Read, J., Härter, M., & Schäfer, I. (2018). “Learning how to ask”: Effectiveness of a training for trauma inquiry and response in substance use disorder healthcare professionals. Psychological Trauma, 10(2), 229-238.
Maté, G., & Maté, D. (2022). The Myth of Normal: Trauma, Illness & Healing in a Toxic Culture. Random House.
Masiero, M., Mazzocco, K., Harnois, C., Cropley, M., & Pravettoni, G. (2020). From individual to social trauma: Sources of everyday trauma in Italy, the US and UK during the COVID-19 pandemic. Journal of Trauma & Dissociation, 21(5), 513-519.
McCann, I. L., & Pearlman, L. A. (1990). Vicarious trauma: A framework for understanding the psychological effects of working with victims. Journal of Traumatic Stress, 3, 131-149.
McChesney, K. (2022). A rationale for trauma-informed postgraduate supervision. Teaching in Higher Education, 29(5). https://doi.org/10.1080/13562517.2022.214546
McClintock, K., Haereroa, M., Brown, T., & Baker, M. (2018). Kia hora te marino – Trauma Informed Care for Māori. Te Rau Matatini.
Mental Health Coordinating Council. (2018). Because mental health is everyone’s business: Annual Report.
Menzies, K. (2019). Understanding the Australian Aboriginal experience of collective, historical and intergenerational trauma. International Social Work, 62(6), 1522–1534.
Meredith, P., Yeates, H., Greaves, A., Taylor, M., Slattery, M., Charters, M., & Hill, M. (2018). Preparing mental health professionals for new directions in mental health practice: Evaluating the sensory approaches e‐learning training package. International Journal of Mental Health Nursing, 27(1), 106-115. https://doi.org/10.1111/inm.12299
Metzler, M., Merrick, M., Klevens, J., Ports, K., & Ford, D. (2017). Adverse childhood experiences and life opportunities: Shifting the narrative. Children and Youth Services Review, 72, 141-149.
Ministry of Health. (2017). Mental Health and Addiction Workforce Action Plan 2017-2021.
Moffitt, T. E., & the Klaus-Grawe 2012 Think Tank. (2013). “>Childhood exposure to violence and lifelong health: Clinical intervention science and stress-biology research join forces. Development and Psychopathology, 25(4), 1619-1634.
Morrissey, J. P., Ellis, A. R., Gatz, M., Amaro, H., Reed, B. G., Savage, A., Finkelstein, N., Mazelis, R., Brown, V., Jackson, E. W., & Banks, S. (2005). Outcomes for women with co-occurring disorders and trauma: Program and person-level effects. Journal of Substance Abuse Treatment, 28(2), 121–133.
Muskett, C. (2014). Trauma-informed care in inpatient mental health settings: A review of the literature. International Journal of Mental Health Nursing, 23(1), 51-59.
Niimura, J., Nakanishi, M., Okumura, Y., Kawano, M., & Nishida, A. (2019). Effectiveness of 1‐day trauma‐informed care training programme on attitudes in psychiatric hospitals: A pre–post study. International Journal of Mental Health Nursing, 28(4), 980-988.
Nizum, N., Yoon, R., Ferreira-Legere, L., Poole, N., & Lulat, Z. (2020). Nursing interventions for adults following a mental health crisis: A systematic review guided by trauma-informed principles. International Journal of Mental Health Nursing, 29(3) 348-363.
Palfrey, N., Reay, R. E., Aplin, V., Cubis, J. C., McAndrew, V., Riordan, D. M., & Raphael, B. (2018). Achieving service change through the implementation of a trauma-informed care training program within a mental health service. Community Mental Health Journal, 55(3), 467-475.
Patterson, R., Durie, M., Disley, B., & Tiatia-Seath, S. (2018). He Ara Oranga: Report of the government inquiry into mental health and addiction.
Pfeiffer, K. M., & Grabbe, L. (2022). An approach to trauma‐informed education in prelicensure nursing curricula. Nursing Forum, 57(4), 658-664.
Pihama, L., Smith, L. T., Evans-Campbell, T., Kohu-Morgan, H., Cameron, N., Mataki, T., Te Nana, R., Skipper, H., & Southey, K. (2017). Investigating Māori approaches to trauma informed care. Journal of Indigenous Wellbeing, 2(3),18-31.
Pihama, L., Smith. S., Cameron, N., Te Nana, R., Kohu-Morgan, H., Skipper, H., & Mataki, T. (2020) He Oranga Ngākau: Māori approaches to trauma-informed care. Te Kotahi Research Institute.
Pihama, L., & Tuhiwai Smith, L. (2023). Māori and Indigenous approaches to trauma and healing. In L. Pihama & L. Tuhiwai Smith (Eds.), Ora: healing ourselves – Indigenous knowledge healing and wellbeing (pp. 15-27). Huia Publishers.
Reid, C., Bennetts, S. K., Nicholson, J. M., Amir, L. H., & Chamberlain, C. (2023). Rural primary care workforce views on trauma‐informed care for parents experiencing complex trauma: A descriptive study. Australian Journal of Rural Health, 31(1), 98-113.
Royal Australian & New Zealand College of Psychiatrists (RANZCP). (2020). Position statement 100: Trauma-informed practice.
SAMHSA. (2014a). SAMHSA’s concept of trauma and guidance for a trauma-informed approach.
SAMHSA. (2014b). Trauma-informed care in behavioral health services: A treatment improvement protocol. US Department of Health and Human Services.
Siegel, D. (2012). Pocket guide to interpersonal neurobiology: An interactive handbook of the mind. Norton and Company.
Skarupski, K. A., Parisi, J. M., Thorpe, R., Tanner, E., & Gross, D. (2016). The association of adverse childhood experiences with mid-life depressive symptoms and quality of life among incarcerated males: exploring multiple mediation. Aging & Mental Health, 20(6), 655-666.
Slatyer, S., Craigie, M., Rees, C., Davis, S., Dolan, T., & Hegney, D. (2018). Nurse experience of participation in a mindfulness-based self-care and resiliency intervention. Mindfulness, 9(2), 610-617.
Smallwood, R., Woods, C., Power, T., & Usher, K. (2021). Understanding the impact of historical trauma due to colonization on the health and well-being of Indigenous young peoples: A systematic scoping review. Journal of Transcultural Nursing, 32(1), 59-68.
Stokes, Y., Jacob, J.-D., Gifford, W., Squires, J., & Vandyk, A. (2017). Exploring nurses’ knowledge and experiences related to trauma-informed care. Global Qualitative Nursing Research, 4.
Sundborg, S. A. (2019). Knowledge, principal support, self-efficacy, and beliefs predict commitment to trauma-informed care. Psychological Trauma, 11(2), 224-231.
Sweeney, A., Clement, S., Filson, B., & Kennedy, A. (2016). Trauma-informed mental healthcare in the UK: What is it and how can we further its development? Mental Health Review Journal, 21(3), 174-192.
Sweeney, A., Filson, B., Kennedy, A., Collinson, L., & Gillard, S. (2018). A paradigm shift: Relationships in trauma-informed mental health services. BJPsych Advances, 24(5), 319-333.
Te Pou o te Whakaaro Nui. (2018). Trauma-informed care: Literature scan.
Te Rau Ora, Le Va, Werry Workforce Whāraurau, & Te Pou. (2021). Weaving together knowledge for wellbeing: Trauma informed approaches [Fact sheet]. Te Pou.
Van der Kolk, B. (2005). Developmental trauma disorder: Towards a rational diagnosis for chronically traumatized children. Psychiatric Annals, 35, 401-8.
Wirihana, R., & Smith, C. (2014). Historical trauma, healing and wellbeing in Māori communities. MAI Journal, 3(3).
Wirihana, R., & Smith, C. (2019). Historical trauma, healing and well-being in Māori communities. In C. Smith & R. Tinirau (Eds.), He rau murimuri aroha (pp. 3-16). Te Atawhai o te Ao: Independent Māori Institute for Environment & Health.
Woo Baidal, J., Locks, L. M., Cheng, E. R., Blake-Lamb, T. L., Perkins, M. E., & Taveras, E. M. (2016). Risk factors for childhood obesity in the first 1000 days: A systematic review. American Journal of Preventive Medicine, 50(6), 761-779.
Yatchmenoff, D. K., Sundborg, S. A., & Davis, M. A. (2017). Implementing trauma-informed care: Recommendations on the process. Advances in Social Work, 18(1), 167-185.
Zhang, J., Wang, X., Xu, T., Li, J., Li, H., Wu, Y., Li, Y., Chen, Y., & Zhang, J. (2022). The effect of resilience and self‐efficacy on nurses’ compassion fatigue: A cross‐sectional study. Journal of Advanced Nursing, 78(7), 2030-2041.
Daily doses – uncut news
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


