
 |
About the author:Merian Litchfield, RN, PhD, is an academic-at-large, researcher, educator and consultant. |
||
Abstract
Access to nursing is at the core of health care in civilised societies. This paper is about naming, framing and claiming nursing’s contemporary significance for health and people’s lives through research. I argue that a nursing paradigm, with its historial ethos of caring and humanness, identifies and differentiates nursing’s perspective on health, reframing the paradigm of practical expertise. Drawing on my experience in research, I establish my rationale for nursing as a paradigm that frames “research as-if practice”, as participatory. Through research, each nurse, as practitioner/researcher, evolves and presents findings as practice wisdom: the coherence of the knowing and the doing aspects of nursing. The significance of nursing is explained as being its knowledgeable practitioners – their methodology is not deterministic, and involves “what can be” for all participating. The nursing voice comes from the collective. The need for kōrero, and for a succinct phrase indicating the distinctly nursing perspective of health in Aotearoa/New Zealand as a reference point are emphasised.
Key words
nursing knowledge, methodology, perspective of health, nursing voice, technology, practical expertise, practice wisdom
Introduction
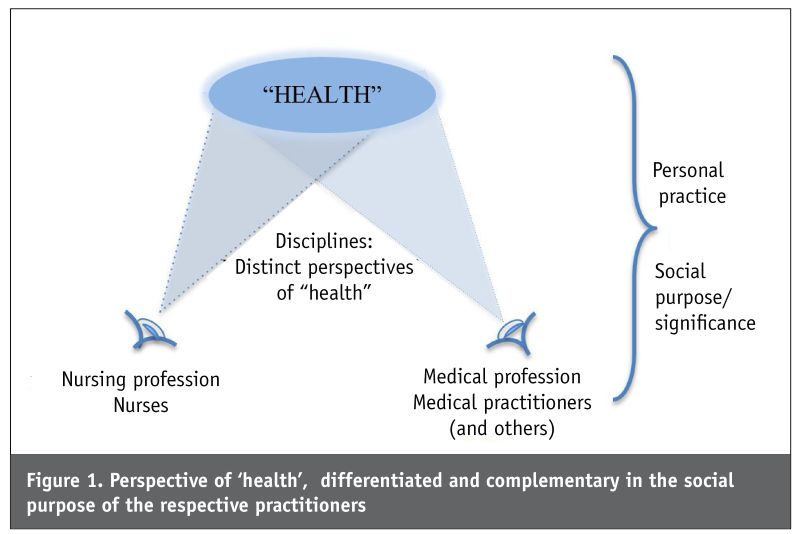
I WAS CHALLENGED TO write this paper to bring some coherence to my career-long efforts to say what it is about nursing that is essential to the health, health care and lives of people here in Aotearoa/New Zealand. Early in my career, I worried about what I should know as a nurse tutor. Through my academic studies to find out, I became convinced that nursing is a discipline in its own right, but I couldn’t explain it. So, many years ago, I drew a diagram (Figure 1, opposite page) that would serve to focus conversations with nurses. I have continued to elaborate (and question) my thinking and language with reference to the diagram. I present it here with my explanation – to date – to bring the focus to research and methodology.
What we as nurses know, from experience, about the significance of nursing cannot be explained as just an adjunct of another discipline. There is a vast literature published around the world by nurses as scholars and researchers that has offered a myriad viewpoints of this since Florence Nightingale. My diagram and explanation echo many; it is part of the global and evolving dialogue that has sustained nursing through its history. In one of her editorials, Sally Thorne (2018), Canadian editor of the journal Nursing Inquiry, cited a number of authors using a similar metaphor to mine to distinguish nursing’s “unique and distinctive” perspective. Wrestling with many of the same concerns, she wrote: “This ‘angle of vision’ depicts a particular stance toward the universe of interest, shaped by certain ways of knowing and perceiving”.
This is a diversion from the current emphasis on analyses of workforce. I present a view of research as concerned with “what can be” when the significance of nursing as “practice wisdom” is acknowledged. It is a step back from the current “what is” concerns with nurse roles and positions: nurses being “fit-for-purpose” in the health services that employ them. I see nurses as knowledgeable practitioners whose significance for health and people’s lives is recognised directly in the design and delivery of health-care systems – not defined by those systems. Practice, in its methodology, is at the core of nursing’s paradigm where, through research, we bring coherence to the knowing and the doing aspects of nursing.
With reference to the diagram (Figure 1), I address each of the components before eventually reaching the topic of research and methodology. I have to first establish my rationale for nursing as a distinct practice discipline, significant because of its “unique and distinctive” perspective on health: what knowledgeable nurses pay attention to, what they do about it, and what is achieved by it. A definitive methodology for nurses in the conventional sense should not be expected.
I refer to nurses as those who have been credentialed with the legally protected title of nurse when entered on that register (RNs). They might be practising directly with patients/consumers, educators or managers. The profession refers to the bodies representing RNs and those in allied nurse roles. The perspective that gives nursing its contemporary social purpose is a professional matter.
The ‘health’ focus
“Health is everybody’s business”.
Bee Salmon, NZ nursing academic pioneer, speaking to Auckland nurses in 1971 (Salmon, 1983).
“Nurses, individually and collectively, are responsible for representing ourselves as expert capable members of a profession that is the core of NZ’s health system”.
Patricia McClunie-Trust, nursing educator, scholar and research leader; editor of Kaitiaki Nursing Research (McClunie-Trust, 2021)
The starting point is “health”. This is our overall sphere of interest. In my diagram, “health” is in inverted commas to convey that although it is a word familiar in the conversations of our everyday lives, it is packed with a complexity of meanings that have evolved through time; it has been explored, defined and debated in the literature. It is accepted globally as a vital facet of life and living at the centre of government in civilised societies. The World Health Organization (WHO) has repeatedly led international collaboration to redefine it for relevance in contemporary contexts, to urge the international sharing of information and experience and inspire whatever action each nation state decides will improve the quality of life of its citizens. As such, “health” is a reference point for international dialogue that we must participate in – from our own national and nursing standpoints.
In Aotearoa/New Zealand, we know that cultural perspectives vary the meaning of “health” – this is vital to how we live in our world and experience our nationhood. We know the conventions of health care shaped by the historically-dominant western perspective have not benefited citizens equitably. But also we are part of the growing public consciousness that the meaning of “health” that drives health care should include other perspectives. Recognising Te Tiriti o Waitangi as the foundation of our nationhood, metaphors for “health” and te reo Māori have shaped how our nation addresses it: Mason Durie’s Te Whare Tapa Whā and Te Pae Māhutonga (Ministry of Health, 2017a), and Rose Pere’s Te Wheke (Ministry of Health, 2017b). Irihapeti Ramsden (1990) introduced “kawa whakaruruhau” (cultural safety) to embed culture and equity as fundamental to “health”. And, of course, every one of us has our own meaning for “health”, elaborated through living and chatting together, being exposed to the media and experiencing health care.
Nurses bringing their own perspective to “health” and research must take into account these current renderings and debates around them – but not be confined by them. The relevance of the perspective is personal for practitioners/researchers, and is also framed by the collectives that assert the professional social purpose of their discipline.
Complementary perspectives of ‘health’
“Experience teaches me that nursing and medicine must never be mixed up. It spoils both.”
A letter from Florence Nightingale to a medical academic friend, 1869 (Baly, 1997, p.77)
In the diagram, I use eyes to represent the sources of two perspectives giving “health” its meaning, according to separate disciplines. Particularly important for understanding the diagram and the following discussion is that the discipline perspectives are discrete: the perspectives do not merge (a two-dimensional diagram can’t show this). When recognised as distinctly different, disciplines can then be considered complementary in addressing “health” matters. This provides for a more inclusive kōrero and a richer conceptualisation as foundation for health-service systems.
Medicine is the discipline for comparison with nursing. When we talk about health care being inter- and multi-disciplinary, we must assume that nursing is a discipline – essential alongside medicine, and with its own identifying social purpose. But as noted above, the predominant perspective of “health” has determined the conventions of health care. The discourse expresses the highly-respected social purpose of medicine: the amazing potential of discoveries in medical science and technology. Medical research produces the form of knowledge considered the core of health care; its assumptions of “health” deeply convincing as the hegemony of contemporary service systems, its conventions resilient and self-reinforcing. The methodology is science, empirical – objectifying, to be prescriptive. This is the loudest voice of health-care. Importantly, the methodology developing the discipline of medicine is philosophically consistent with the methodology of its practitioners.
To differentiate perspectives of “health”, we look for relevant language for the distinct social purpose of each. For the medical perspective, I have taken the definition of medicine from the succinct and widely accessible English dictionary on my computer (www.lexico.com: Powered by Oxford. Retrieved 25.10.21): “The science or practice of the diagnosis, treatment, and prevention of disease”. I extrapolate from this: the practitioners of medicine give “health” its everyday meaning in terms of the cure and control of disease, assuming its scientific methodology.
For nurses, it has been difficult to similarly convey “a professional practice”, to find the language for its social purpose in terms of direct significance for health and people’s lives. It is not medicine and is not just what anyone can “do”. To people without the qualification and experience of a nurse, nursing is commonly referred to in terms of support for the predominant “health” purpose, that is nurses as part of the generic “medical workforce”. This is emphasised by Canadian journalists Buresh and Gordon (2013), who urged nurses to broadcast what they do. But given the hegemony of our health system, the workforce is constructed (or minimised) around quality and economic decisions, according to the medically-oriented social purpose of the system.
In this light, we need to consider the “doing” work defining the workforce, before looking at what “health” benefit comes from the nursing perspective.
Practical expertise
“We are on the brink of a period of fundamental and irreversible change in the way that the expertise of . . . specialists is made available in society. Technology will be the main driver of this change. And, in the long run, we will neither need nor want professionals to work in the way that they did in the twentieth century and before.”
Susskind & Susskind, academics of Oxford University, 2017, p.1
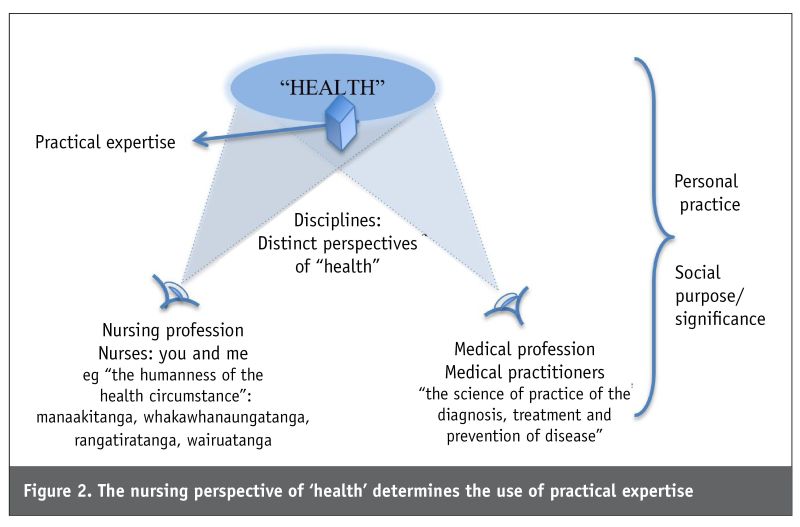
Irrespective of perspective of “health”, there are many activities now not exclusive to any one workforce group or profession. I have inserted a three-dimensional box into my diagram (Figure 2, below) to symbolise the collection of all the actions and skills used in the provision of health care. They include procedural tools and instruments (including assessment formats), checklists, decision-supports, flow-charts, guidelines, protocols, algorithms. They are the substance of evidence-based competencies, developed, modified and improved through research. Around them, training and quality control programmes have been constructed, inter- and multi-disciplinary.
I have taken the term “practical expertise” from the book by the Susskind father and son duo of Oxford University, in the United Kingdom: The Future of the Professions: How technology will transform the work of human experts (2015). They observe a transformation underway in the production and distribution of the knowledge and expertise once held in the mandated realms of professions: they say the future will be in artificial intelligence, robots and the internet. Having analysed the trend in their own professions of law and economics, and explained this as “dismantling”, they observed the same trend in the other traditional professions. Now “ . . . we cannot afford them, they are often antiquated, the expertise of the best is enjoyed only by a few, and their workings are not transparent.” (p. 3).
The Susskinds argue that “today’s professions should and will be displaced by feasible alternatives” (p. 3). Professional work, they observe, is being demystified and gatekeeping bypassed. Drawing on extensive research, they depict the trend as a “decomposition of professional work” – from the personalised, bespoke craft of professionals in the past, to routinised and increasingly standardised packages of expertise that are being digitised, built into systems and then liberated into the internet to be available in the public arena. Through this process, expertise is extracted and allotted to whomever is best suited. Given the financial incentive associated with the delegation of practical expertise, in parts, down the line of cost containment, the process is “commodification”. Eventually and inevitably, the items of practical expertise reach the realm of increasingly capable machines.
It is not difficult to see this trend in our health sector, with nurses major players. Professional practices are changing as components of their jobs are delegated to, or claimed by, others no longer needing the full depth and breadth of knowledge and competency once believed essential. With technology expanding, our health workforce has been diversifying into specialisms, opening new roles for health-care workers with their own protocols, credentialing, job descriptions etc (eg delivering meal trays to hospital patients; hysteroscopy). Discoveries are in the media daily and marvelled at in everyday conversations. The box of practical expertise is expanding unstoppably. For now, it is confined by and reinforcing the hegemony of the health system.
The Susskinds (2015) are confident that people will be better placed to access, afford and benefit from the advances in science and technology. But we see the impact of the increasing fragmentation of the health-care people receive, and envisage the growing vacuum where the human face and human touch used to be, when the practical expertise becomes an end itself. And unrest comes from the competition around who does – or should – do what tasks. In my diagram (Figure 2), the box is set within the perspective spheres of both nursing and medicine. We often “do” the same tasks. However, we know nursing is more than just the practical expertise. So nurses, like others in the workforce, are called to convincingly articulate why, because of their nursing perspective of “health”, they should usefully incorporate items of practical expertise in practice.
The nursing perspective
“The humanness of life is the natural setting for nursing . . . the nurse brings to a situation a language of herself, her peculiar wit and skill and comprehension of things.”
Bee Salmon, in her keynote address to the 1968 ICN Congress, Montreal, Canada (Salmon, 1983)
“Cultural safety requires that nurses care for people regardful of those things which make them unique”. (emphasis original)
Irihapeti Ramsden (Ngāi Tahu, Rangitāne), nurse educator and consultant, author of Kawa Whakaruruhau: Guidelines for Nursing & Midwifery Education (Papps & Ramsden, 1996, p.491)
“I would love to see more nurses initiate real conversations with focus on the person in their care, rather than referring them on to somebody else. What we say as a nurse is like sowing a seed – every opportunity matters.”
Isabelle Sherrard, RN, letter to the editor, Kaitiaki Nursing New Zealand, October 2021
Whereas nurses readily engage with medical colleagues (and others in the health workforce) about the medical aspects of patient care, we know there is so much more to nursing that is unsaid and unacknowledged. So here I differentiate a nurse’s perspective of “health”, which is just as essential: to name and claim it as complementary so that “health” is addressed holistically.
To start, I again refer to my computer dictionary for a succinct definition of nursing that is publicly recognised and commonly accessed: “The profession or practice of providing care for the sick and infirm” (www.lexico.com: Powered by Oxford. Retrieved 25.10.21). These dictionary definitions of nursing and medicine (see above) are closely matched in words and syntax, which makes them useful for comparison. Both are understood as practice professions. Nursing is concerned with care, in place of science, and focused on the sick and infirm, in place of disease. I take from this that nursing is seen as attending to people’s “health”-related predicaments as an emotional engagement; medicine is defined by its scientific knowledge used in a practice that is deterministic, its purpose the cure and control of disease. The ethos differs: process vis-à-vis outcomes. The perspective of “health” differs – the perspective that determines what practitioners primarily pay attention to, and how they address it (and what funding there is for it).
The word “caring” to identify the nursing ethos is familiar to us. It became an explicit connector for international conversations among nurses, bringing solidarity and a sense of professional identity. In New Zealand, from the 1960s, “caring” was used to identify and define nursing in core statements of the New Zealand Nurses’ Association (NZNA): “. . . nursing is a specialised expression of caring . . .”. (NZNA, 1976, 1985). New Zealand nursing scholar and educationist Bee Salmon had earlier worded the nursing ethos as “warmth, understanding and compassion . . . the well springs of the profession we represent” in her keynote to the 1969 International Council of Nurses (ICN) congress in Montreal, titled What Comes from the Heart Goes to the Heart (Salmon, 1983). Much earlier, Grace Neill (Neill, 1961), who wrote and implemented the 1901 Nurse Registration Act, in her keynote to the international gathering of nurses that was the precursor to ICN, said of the nurse: “upon her patience, skill and gentle tendency rest the comfort and well-being . . . ” This is our history, of an enduring ethos which is the source of our identity and social purpose as “nurses” today (albeit framed in ways and in language relevant for the day): he tangata; it is people. However, the usefulness of the word “caring” has been fading. It is no longer adequate for conveying either a distinct nursing perspective or what nurses do in today’s context (Allen, 2014; Buresh & Gordon, 2013). So now we look for some wording for contemporary relevance, that each of us can identify with, and to spark the kōrero to connect us.
In 2006, my friend and colleague Helga Jónsdóttir, professor in the School of Nursing, University of Iceland, and I collaborated on a publication to contribute to the debate on the focus of the discipline of nursing. We agreed on a phrase: “the humanness of the health circumstance” (Litchfield & Jónsdóttir, 2006). As a phrase this was just a reference point in common, with enough meaning for each of us to prompt reflection on our own work, and to advance our respective agenda.
Here is my “take” on the phrase, coming from my research experience and academic study. The words were adequate; the syntax was what gave it meaning for the way I saw nursing. I could see in it the historically consistent trend of ethos. As a reference point for “health circumstance”, it allowed me to take account of the knowledge of what is currently considered “health” from the predominant perspective and also the complexity of its contexts. What I wanted to acknowledge as the uniqueness of experience, everyday living with disease and disability, practice as relational and contingent, could be elaborated for nursing. And also, to consider the presence of the nurse in the partnership, genuinely engaging with people about what matters to them. I thought it would draw practitioners, educators and managers into the kōrero with researchers, with their various “takes” on nursing’s social purpose and what needs to be done.
This wording would give a focus for discussion of nursing education, practical expertise, and how nurses work with advancing technology. It would help to challenge habitual thinking, inspire study and innovation for new roles, irrespective of service and sector divisions, and the divisions of personal and population health-care. It surely would give a pointer to a person-centred model of care.
The phrase draws our attention to values and language. In Aotearoa/New Zealand, te reo and English give vitality to the relational and contingent nature of partnership. Personal values in my work that I saw represented in the phrase were: a sense of belonging and of “the presence of past and future” (Litchfield, 1999). Partnership, participation and protection represent “regardful” values we all want for our bicultural nationhood and a “culturally safe” multicultural society. Manaakitanga, whakawhanaungatanga, rangatiratanga, wairuatanga are particularly meaningful for explaining “the humanness of the health circumstance”; they do not need definitions to connect us into kōrero about nursing in Aotearoa/New Zealand. This is the language of the current NZNO definition of nursing for its work (Clendon, 2011).
I have found the phrase useful when I talk with nurses about the significance of their practice. I have asked them to explain what they do. I have seen them somewhat startled by the strangeness of both the question and the language; they pause and concentrate hard to find wording for their work. (Nurses are more used to talking about what they do in terms of the medical discipline and workforce roles; to escape from it requires mental effort and overcoming the fear and embarrassment of not having a ready answer.) But also I have repeatedly seen the great and unexpected pleasure of insight when they realise how important their nursing has been – for health and people’s lives. This is foundation for engaging in nursing research. And isn’t it the educative/learning process?
I write about the phrase here, in my words, not to justify or persuade. Rather it is to emphasise that a phrase is essential as a reference point for the kōrero and for the research through which we explain practice and create the nursing voice we need and want: to focus our efforts to articulate nursing. To be inclusive, the phrase must have as few words (meaning-laden) as possible, to accommodate the diversity and uniqueness of personal practice. It must also have the syntax that helps us give a distinctive nursing meaning to the words, our “mindful” (non-deterministic) ethos, the wairua and aroha of cultural safety. Vitally, it must come readily to our minds anywhere we talk to others about nursing. It must be primarily meaningful for the people of Aotearoa/New Zealand, but also for us to engage in the international nursing community. That is, to be readily recognisable, in its essence, as the nursing people need, want and can see as practicable.
I have been deliberate in arguing that we use a phrase – without a verb. How we understand knowledge involves how we use it in practice. This is the issue to be addressed in discussion of distinctly nursing research and its methodology.
The nursing paradigm of research and methodology
“Nursing research is undertaken by nurses. It is a process of systematic enquiry, the purpose of which is to contribute to the shaping of nursing practice within its changing context.”
NZNA Statement on Nursing Research, 1990
“It behoves us [nurses] not to be told by other people what we should be doing – listen certainly – but to define and develop our own practice through research”.
From a 2007 interview with Bernie King, first New Zealand RN to earn a PhD (1981), later senior research officer in NZ Department of Health (Litchfield, 2009, p.16).
“Cultural Safety theory . . . in essence puts the nurse as the focus of insight and change, not the patient . . . It is essential that . . . we value and respect our own experience . . .”
Irihapeti Ramsden, RN (Ngāi Tahu, Rangitāne) (2001, p.24).
In my diagram, there are two paradigms for the research relevant to nursing. One is the box of practical expertise substantiated through research and assuming the methodologies of science framed by the dominant medically oriented perspective and purpose; it is the foundation for evidence-based/informed activities. The other is the nursing paradigm, its discipline created by the perspective of nurses as individual human beings and as a professional collective.
If “humanness” identifies a nurse’s perspective of “health”, then it is the relational, contingent – and dialogic – core of nursing practice, personalising practical expertise, that is to be studied as nursing knowledge. As nursing researchers, our interest is the practice partnership: our personhood – who we are and what we know – coming together with the personhood and health predicament of others, as the nursing endeavour (Jónsdóttir et al., 2004). This differentiates the perspectives as paradigms.
In the literature, there are many thoroughly-explored renderings of two paradigms for nursing research. Here I cite Afaf Meleis (2017) who, every five years since 1985, has intensively reviewed the literature to describe trends in the discipline of nursing in her widely-cited book Theoretical nursing: development and progress. In her most recent edition, she envisaged an emergent generation of nurses researching from “two possible models” that will continue into the foreseeable future. She hasn’t named them, but how she has contrasted them seems to fit with the paradigms I am conveying in my diagram. However, like others, Meleis presents her models as quite discrete paradigms, their methodologies used in parallel as options for researchers in their respective cadres. Rather, in my diagram, I point to nursing as a paradigm itself: one paradigm with its methodology bringing fresh meaning to the box of practical expertise already embedded in the many methodologies of competency. The following is a very condensed rationale.
Practical expertise paradigm
Knowledge is underpinned by the conventional methodologies, both quantitative and qualitative. They are definitive and prescriptive, to produce the form of knowledge required for the workforce to achieve the desired outcomes of the “health” service: to do better. The findings of researchers are made available to be operationalised by practitioners and others; to be confirmed, refuted or modified and built on in new research; methodology and its products are legitimised through the conventions of critique. A whole academic field of “knowledge translation”, and a career role as “knowledge broker” have emerged. This form of knowledge is depersonalised and its use self-reinforcing in trends: it’s a ‘hard boundary’ between knowledge and its application/use in “health” practices.
Nurses have contributed voluminously to the contents of this box of practical expertise; they have structured research and teaching programmes around them. People have benefited from the proficiency of nurses and others in the workforce drawing on the evidence to inform their work. Nurses must continue with this essential contribution, using whatever methodology serves their practical expertise intent. But a nurse’s research from a nursing paradigm reframes the interface of this form of knowledge and its relevance in people’s lives.
The nursing paradigm
As for other disciplines, distinctly nursing research calls for methodology to express the premises of the nursing perspective of “health”. The significance of nursing lies in a relational, contingent form of practice focused on people’s lives, so the methodology is the way we develop knowledge as it evolves in the reality of our practice experience, along with all the participants (Jónsdóttir et al., 2004, Litchfield, 1999): the humanness/mindfulness of partnership as practice.
To give our methodology a genre that links it into the wider research literature, I refer to it as participatory (Litchfield & Jónsdóttir, 1999). Philosophical foundations for a range of participatory methodologies emerged in the social science literature a long time ago and the relevance for nursing was quickly recognised, although not without controversy. US nurse theorist Margaret Newman (1991, p.100) explained to a sceptic: “research is practice” means “the form that nursing research takes is the form of practice: a real relationship between nurse (researcher-practitioner) and client focusing on a real concern of nursing practice” (emphasis original). Nursing research requires our own rendering.
So in the nursing paradigm, identified by its “health” perspective with social purpose, research is the process by which the methodology itself is the findings. Presented as a narrative of process, this is practice wisdom. It is what happened through the process and what eventuated, not predetermined: the humanness of the partnership (Litchfield, 1999). “The nurse (is) the focus of insight and change” (Ramsden, 2001, p.26). In this paradigm, the box of practical expertise is re-construed as a library of current conventions, “items” critiqued for usefulness as part of the uniqueness of the partnership, in context. Here, practical expertise is actually integral to the “health circumstance” that is partnership. It is personal practice, a nursing process that is opportunity for “health” to be understood as “what can be”: what is to be done by any and all participants.
Since “research” takes its contemporary meaning and legitimacy within established ethics guidelines, committee approval, funding, publication, conference presentations etc, I emphasise that this endeavour is “research”, not to be dismissed as the expected everyday development of practice: it is “research as-if practice” (Litchfield, 1999; Jonsdottir, 2007). Of course, as such it needs “research” design parameters.
However, the presentation of a nurse researcher’s narrative of practice wisdom – which is personal – does not itself develop the discipline. It is when the narratives of practice wisdom are brought into the collective dialogue that the discipline evolves. The nursing discipline is a dialogue. It is through our kōrero as knowledgeable nurses, here and now, that we can seek the unity of diversity for a nursing voice substantiated though research. In our hui and forums, we do the mahi on the meaning of Te Tiriti for “health”, on Kawa Whakaruruhau and Cultural Safety in Nursing (Ramsden, 1990; Roberts, 2019), we question our ethics and develop confidence.
Conclusion
So, nursing does have a methodology. It is the way nurses become knowledgeable, bringing coherence to “knowledge” from all sources and the experience of nursing. It cannot be defined like the conventions of research in the health field. In this sense, nursing is methodology. Nursing is a paradigm.
The conceptualisation I have diagrammed is embedded in our Aotearoa/New Zealand nursing turangawaewae, but the thinking echoes through international nursing literature. Meleis (2017) referred to the same elements and their significance as she pondered the future of nursing theory and research: “By being clear about our mission, our values and the models we choose to use for knowledge development, we are empowering ourselves to empower our consumers.” (p.426). From my stance presented here, I add that nurses and consumers are simultaneously empowered through the process of research-as-if-practice.
I acknowledge the twist of mind involved in looking at nursing research in this way. There is much to be questioned and new ideas to be developed. My explanation is necessarily pared down and superficial. And I am writing as just one reflecting academic-at-large, using my language as best I can, here and now. I hope the diagram prompts kōrero useful to substantiate the vital voice of nursing in health care – where knowledgeable nurses should be free to nurse in new ways in response to changing need, and to claim the conditions required for it. But, for this, there is real need for hui and forums where we can collectively settle on and repeatedly review a phrase, simple and brief, as an identifying reference point for our individual and collective efforts.
Nursing research, when we see that it is and has a methodology with social significance, gives us our voice. Canadian Sally Thorne (2018) reminded us: “a shared voice is fundamental to our public trust”. Our research is how NZNO’s belief about the future can be realised: “Nurses will shape the future of health in this country, we will be recognised for the difference we make in people’s lives, and we will work together as a profession to achieve this”. (Clendon, 2011).
References
Allen, D. A. (2014). The invisible work of Nurses: Hospitals, organisation and healthcare. Routledge.
Baly, M. (1997). As Miss Nightingale said . . . Florence Nightingale through her sayings – a Victorian Perspective (2nd ed.). Bailliere Tindall.
Buresh, B., & Gordon, S. (2013). From silence to voice: what nurses know and must communicate to the public (3rd ed.). Cornell University Press.
Clendon, J. (2011). 2020 & beyond: A vision for nursing. Te mua I te tau. Rua mano rua tekau. He tirohanga mo nga tapuhitanga. NZ Nurses Organisation.
Jónsdóttir, H., Litchfield, M., & Pharris, M. D. (2004). The relational core of nursing practice as partnership. Journal of Advanced Nursing, 47(3), 241-250.
Jonsdottir, H. (2007). Research-as-if-practice: A study of family nursing partnership with couples experiencing severe breathing difficulties. Journal of Family Nursing, 13(4), 443-60.
Litchfield, M. (1999). Practice wisdom. Advances in Nursing Science, 22(2), 62-73.
Litchfield, M. (2009). To advance health care: The origins of nursing research in New Zealand. NZNO.
Litchfield, M., & Jónsdóttir, H. (2006). A practice discipline that’s here and now. Advances in Nursing Science, 31(1), 79-92.
McClunie-Trust, P. (2021). Viewpoint: Pandemic’s impact on the profession. Kaitiaki Nursing New Zealand, 27(3), 13-15.
Meleis, A. I. (2017). Theoretical nursing: Development and progress (6th ed.). Lippincott Williams & Wilkins.
Ministry of Health. (2017a). Māori health models – Te Whare Tapa Whā.
Ministry of Health. (2017b). Māori health models – Te Wheke.
Neill, J. O. C. (1961). Grace Neill: The story of a noble woman. N. M. Peryer Ltd.
New Zealand Nurses Association. (1976). Policy statement on nursing in NZ: New directions in post-basic education.
New Zealand Nurses Association. (1985). Nursing – A social policy statement.
New Zealand Nurses Association. (1990). Statement on Nursing Research.
Newman, M. A. (1991). Dialogue on a research issue: The research-practice relationship. Nursing Science Quarterly, 4(3), 100-101.
Papps, E., & Ramsden, I. (1996). Cultural safety in nursing: The New Zealand experience. International Journal for Quality in Health Care, 8(5), 491-497.
Ramsden, I. (1990). Kawa Whakaruruhau: Cultural safety in nursing education. Ministry of Education.
Ramsden, I. (2001). Improving practice through research. Kai Tiaki Nursing New Zealand, 7(1), 23-26.
Roberts, J. (2019). Kawa Whakaruruhau – has its intent been lost? Kai Tiaki Nursing New Zealand, 20(11), 14-15.
Salmon, E. B. (1983). A profession in transition. C. L. Bailey Nursing Education Trust.
Sherrard, I. (2021). Letter to the Editor: Treasures in September issue. Kai Tiaki Nursing New Zealand, 27(9), 5.
Susskind, R., & Susskind, D. (2015). The future of the professions: How technology will transform the work of human experts. Oxford University Press.
Thorne, S. (2018). Editorial: In search of our collective voice. Nursing Inquiry, 25, e12266.
Daily doses – uncut news
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


