
Students who took part in the programme, which ran for a year in the Nelson-Marlborough region, reported improved understanding of primary care, cultural safety and family/whānau-centred practice, along with greater confidence and adaptability. Educators and providers noted students’ stronger communication skills and improved workforce readiness, as well as a reduction in placement pressures.
Importance of primary health care
Experiencing health care beyond hospital walls in their clinical placements is essential for nursing students to understand the full patient journey.
Primary health care is a cornerstone of the Aotearoa New Zealand health system, which was highlighted during responses to the recent COVID-19 pandemic and measles outbreaks.
While undergraduate nursing programmes do include clinical placements in primary health, the allocation and emphasis of these vary between institutions and regions, and many students still spend a large proportion of clinical hours in hospitals. This limits students’ opportunities to understand how health care is delivered in primary care settings.1,2
The Nelson Bays Primary Health Organisation (PHO) and rural community health care services partnered with education provider, the Nelson Marlborough Institute of Technology (NMIT), to pilot a hub-and-spoke student placement model to increase the diversity of their primary health care clinical experiences.

Benefits of the pilot included increased placement capacity, reduced burden on individual placement providers and richer and more diverse learning experiences for students that strengthened their workforce readiness and their understanding of culturally safe, whānau-centred practice.3, 4 The trial was was part of the students’ third-year family, whānau and community nursing module.
Why a hub-and-spoke model?
Traditionally, nursing students are allocated to one clinical area or specialty for the duration of their placement. While this can provide continuity, it also limits the range of learning opportunities and puts significant pressure on single providers.
Such siloed placement experiences can restrict the students’ understanding of the whole patient journey and discourage smaller providers from participating due to concerns about the limits of of their resources.3
Hub-and-spoke models have been shown internationally to improve student satisfaction, foster positive perceptions of primary care and increase the health services’ capacity for placements.3
Hub-and-spoke structure
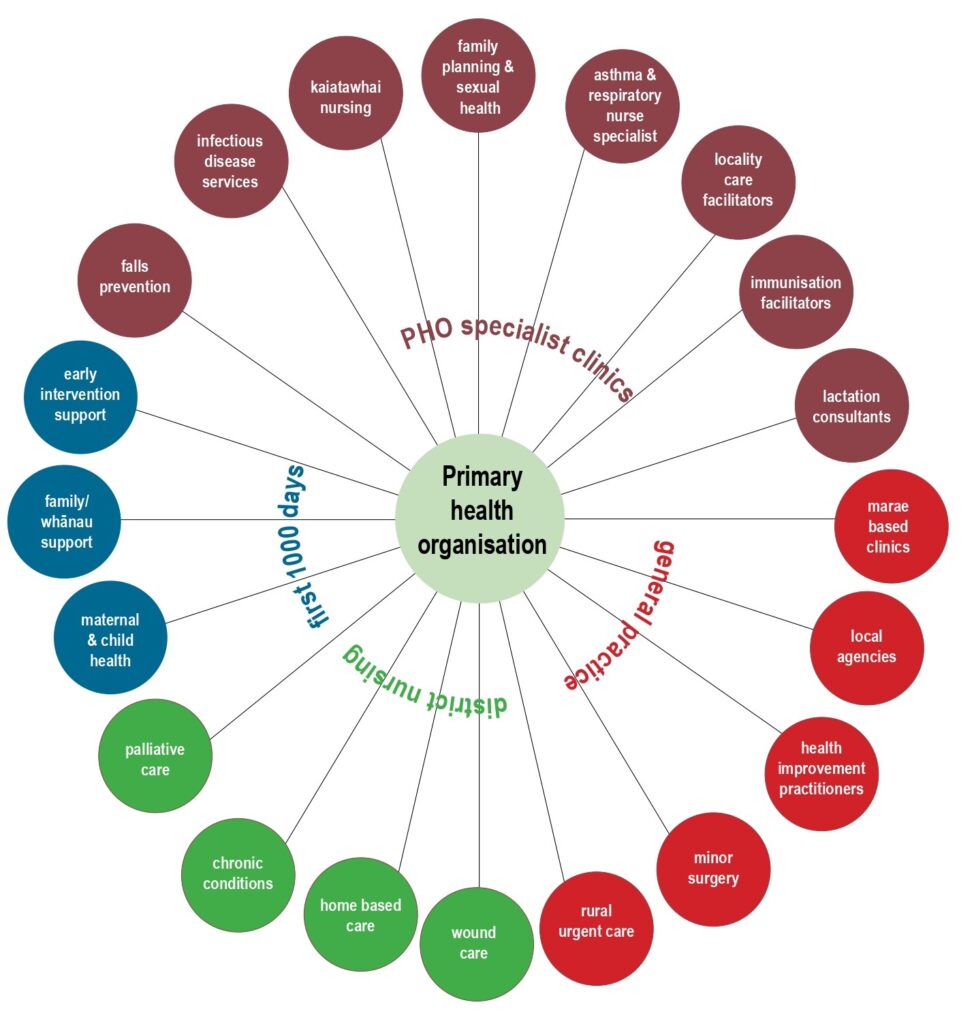
In this pilot, the “hub” for student placements was the Nelson Bays PHO, which provided access to a range of primary health care services and coordinated learning opportunities across its network. From this hub, students rotated through a series of “spoke” placements, each offering distinct perspectives on the delivery of primary health care.
The spoke placements were grouped across four different sectors of the PHO’s services — PHO specialist clinics, general practice, district nursing, and the First 1000 Days (a multidisciplinary service for babies, mothers and whānau) — and the students rotated through these four sectors. In this way, they were able to experience diverse “spoke” placements, including Māori health providers, marae-based clinics and specialist services.
Spokes across the four sectors included:
- Specialist services: Placements with services such as lactation consultants, family planning, a Health Care Homes facilitator and locality care facilitators (who link primary care with specialist and community services for patients with complex needs).
- General practice: Spokes included marae-based clinics in partnership with Māori health providers, local health agencies and rural urgent-care services.
- District nursing: Spokes provided exposure to home-based care, chronic condition management, wound care management, palliative care and community nursing initiatives.
- First 1000 Days: Spokes included placements in the multidisciplinary First 1000 Days collaborative, which brings together Well Child/Tamariki Ora providers, midwives, public health nurses and Māori and community health services. Students gained experience in postnatal care, early childhood health, and whānau-centred support within an integrated, culturally responsive model of care.
At the start of their placement, students were oriented to the hub-and-spoke model at the PHO, starting with a karakia, followed by whānaungatanga with preceptors and hub-and-spoke staff. Students rotated for two to three weeks through each of the hub sectors, accessing a range of spokes in the rural community to gain a broad and varied primary care experience.
The hub-and-spoke model was designed to broaden student learning, strengthen provider collaboration, and deepen cultural engagement in primary health care placements.
Shared supervision across sites reduced the pressure on individual providers while fostering teamwork and continuity of learning.
It enabled students to experience diverse community settings, offering a holistic view of care across general practice, public health, maternal and child health, and outreach services. Shared supervision across sites reduced the pressure on individual providers while fostering teamwork and continuity of learning.
The model also embedded cultural safety principles, aligning with Te Pae Waenga5 and Te Tiriti o Waitangi/the Treaty of Waitangi by promoting equity, partnership and whānau-centred practice.
Some challenges were experienced in the operation of the hub-and-spoke model. These included variations in how ready some spoke sites were to receive students, the demands of coordinating the scheme, and ensuring consistent supervision and assessment. Overall, however, the model showed that meaningful primary care placements can be achieved through shared commitment, flexibility, and strong relationships between education providers and health services.
Evaluation of key findings
Student perspectives
Students reported that the hub-and-spoke model gave them a more authentic understanding of primary health care. Many had assumed public health and general practice were “routine” or a “retirement job,” but rotations revealed the breadth of care, including chronic condition management, health promotion, child health and outreach services.
Placements within the spokes, particularly with kaiatawhai nurses, deepened the students’ understanding of cultural safety and whānau-centred care, reinforcing classroom learning with lived practice.4
One student reflected:
“Seeing how the kaiatawhai worked with whānau made me realise that health care is more than treating illness — it’s about relationships, trust, and culture.”
Another student highlighted their learning goals and the hub-and-spoke model’s emphasis on holistic practice:
“I am hoping to meet all competencies! However, I expect there will be a strong focus on cultural safety and therapeutic relationships. I am hoping to develop good assessment skills that focus on the patient and family/whānau as a whole rather than focusing entirely on symptoms and symptom management as I have experienced in secondary health care.”
Another student commented:
“[I] gained understanding of local health services.”
Students reported increased confidence, adaptability and understanding of the whole patient journey. This mirrored findings in a Scotland study, where hub-and-spoke placements enhanced students’ sense of belonging and connection with communities.6
Educator perspectives
For educators, the hub-and-spoke model provided confidence that students were receiving consistent support while experiencing diverse clinical environments. They saw students develop stronger communication and adaptability skills as they transitioned between settings and engaged with multiple providers.
Some spokes had not previously been used for placements, so these provided new learning opportunities, exposing students to different aspects of nursing in primary care.
One educator noted:
“ . . . from what I saw, the students’ experiences really gave them a clearer sense of the issues affecting patients’ communities.”
These findings align with research showing that students benefit from participating in a variety of workplaces with differing work patterns and methods of care delivery, which enhances their workforce readiness and appreciation of primary care roles.1, 3
PHO and practice perspectives
The PHO viewed the hub-and-spoke model as a way of strengthening relationships across its network. Practices reported that, although hosting students required time and supervision, the rotational structure ensured that no single site carried the full placement load.
By distributing students around the spokes, workload was shared more equitably, enabling staff to engage with learners without compromising service delivery. At smaller rural and kaupapa Māori providers, this arrangement allowed staff to confidently support students while maintaining high quality care.
Providers also said this approach supported workforce development by encouraging nursing students to consider careers in primary health.7 Staff valued the opportunity to share and promote the work occurring in their services, which in turn fostered student interest and sector engagement.
Providers also said this approach supported workforce development by encouraging nursing students to consider careers in primary health.
Challenges and considerations
The model was not without challenges. Coordinating timetables across multiple spokes required careful planning, and students sometimes found frequent transitions between settings demanding. Robust communication between the hub, spokes and NMIT was essential to avoid supervision gaps.
Despite these challenges, most participants felt the benefits outweighed the difficulties. This is consistent with other research noting that while hub-and-spoke models require coordination, they are sustainable when underpinned by strong institutional partnerships.3
Impact on cultural safety and whānau engagement
A notable outcome of the hub-and-spoke model was its contribution to cultural safety. Rotations through kaupapa Māori health providers and marae-based services exposed students to care shaped by a te ao Māori worldview and tikanga (protocol), encouraging reflection and reinforcing whānau-centred practice.
Cultural safety in nursing is best understood as a dynamic practice, built on relationships and situated within communities, which requires nurses to recognise power and privilege.4 This was evident in students’ reflections, which highlighted the relational and trust-based aspects of care.
Primary health care addresses the social determinants of health and supports intergenerational wellbeing.8, 9, 10 This pilot aligns with these principles, embedding students in integrative, community-based services.
Robust communication between the hub, spokes and NMIT was essential to avoid supervision gaps.
Importantly, primary health care encompasses care across the individual’s lifespan. The hub-and-spoke model offered the nursing students opportunities to understand intergenerational health advantage and disadvantage, which consolidated their understanding of the social determinants of health. This aligns with the Nursing Council’s standards,11 which require integration of person and family/whānau-centred care across primary, secondary and tertiary settings.12
Lessons learned and future directions
The hub-and-spoke approach illustrates how nursing education can foster experiential, community-based learning that aligns with Te Tiriti o Waitangi/the Treaty of Waitangi principles, supports inter-professional collaboration and equips students to meet the complex and diverse needs of Aotearoa/New Zealand communities.
The model shows that student placements in primary health care can be expanded through creativity, collaboration and shared responsibility. The model reduced pressure on individual clinical areas, strengthened cultural safety and provided students with experience in the predominant setting in which an individual’s health care is delivered.
Through rotations across the spokes, students developed clinical skills, adaptability, and confidence, while gaining insight into the diversity of primary care services and the importance of culturally safe, family/whānau-centred practice. Educators and providers reported enhanced communication, workforce readiness and engagement with the primary health care sector, supporting students’ future career pathways.
The framework also highlighted areas where the curriculum could be improved and clinical learning experiences for nursing students further developed by strengthening exposure to coordinated, interprofessional models of care.
This model could be scaled up to national level in nursing education.
However, challenges were also identified. These included the need for consistent coordination between education providers and placement sites, equitable resource allocation, and the ongoing mentoring required to sustain quality learning experiences across multiple settings. Ensuring cultural safety and workload balance for preceptors, particularly in smaller or rural practices, remains essential for long-term viability.
Although this pilot only ran for one year, it has had a positive ongoing effect on clinical placements in the Nelson region, opening up new opportunities in primary health, particularly in the PHO. The hub-and-spoke programme opened doors and allowed managers in health providers to see the benefits of taking on students for clinical placement.
This model could be scaled up to national level in nursing education, to improve access to community-based clinical placements, address placement shortages, enrich student learning, and prepare a nursing workforce capable of delivering culturally safe, and community-focused care.
This aligns with Health New Zealand — Te Whatu Ora’s Health Plan ,5 which emphasises the need for a new system of coordinated student placements to meet future workforce demand. Successful expansion requires institutional commitment, robust coordination, and sustainable partnerships between education providers and primary care services.
Recruiting and retaining nurses and allied health professionals in primary health remains vital to addressing inequities and delivering on Te Tiriti o Waitangi/the Treaty of Waitangi commitments.
Karla Breen Rickerby, RN, PhD, is an experienced primary health care nurse, who alternates between primary health work in the Nelson region, and in Aboriginal-run clinics in remote areas of Queensland, Australia.
* This article was reviewed by Anna Askerud, RN, MHSci, DipTchg, PhD, a senior lecturer in the Department of Nursing, University of Otago, Dunedin. She has worked in both primary health and acute care and her special research interest is integrating care of people with long-term health conditions.
References
- van Iersel, M., Latour, C. H. M., van Rijn, M., de Vos, R., Kirschner, P. A., & Scholte op Reimer, W. J. M. (2020) . How nursing students’ placement preferences and perceptions of community care develop in a more ‘community-oriented’ curriculum: a longitudinal cohort study. BMC Nursing, 19(80).
- Betony, K., & Yarwood, J. (2013). What exposure do student nurses have to Primary Health Care and community nursing during the New Zealand undergraduate Bachelor of Nursing programme? Nurse Education Today, 33(10), 1136-42.
- Cleaver, K., Don, C., Chojnacka, I., Essex, R., Weldon, S., & Markowski, M. (2023). A systematic scoping review of undergraduate nursing hub-and-spoke placement models. British Journal of Nursing, 32(5), 252-258.
- Curtis, E., Jones, R., Tipene-Leach, D., Walker, C., Loving, B., Paine, S.-J., & Reid, R. (2025). Refining the definitions of cultural safety, cultural competency, and cultural humility: A systematic review. International Journal for Equity in Health, 24(1), 1-11.
- Health New Zealand/Te Whatu Ora. (2025). Te Pae Waenga: Timely access to quality healthcare 2024-2027.
- Millar, L., Conlon, M., & McGirr, D. (2017). Students’ perspectives of using the hub and spoke model to support and develop learning in practice. Nursing Standard, 32(9), 41-49.
- Hamiduzzaman, M., McLennan, V., Nisbet, G., Jindal, S., Miles, S., Crook, S., Nelson, K., Williams, C., & Flood, V. (2025). Impact of allied health student placements for older clients’ health and wellbeing in primary healthcare settings: A systematic integrative review. BMC Health Services Research, 25, Article 60.
- King, A. (2001). The Primary Health Care Strategy. Wellington, New Zealand: Ministry of Health. https://www.health.govt.nz/publications/the-primary-health-care-strategy
- Durie, M. (2000). Whaiora: Māori health development (2nd ed.). Oxford University Press.
- World Health Organization. (2008). Closing the gap in a generation: Health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health.
- Nursing Council of New Zealand. (2021). Education programme standards for Registered Nurse Programmes.
- New Zealand Government. (2003). Health Practitioners Competence Assurance Act 2003.