
During our second-year clinical inpatient placements, some of us observed that written information, provided in pamphlets and handouts, was effective in facilitating patient education and enhancing health literacy.

Our observations are supported by recent research1, 2, which identified that written information following patient discharge significantly enhances and supports patient health literacy and self-management.
We have seen written information used to educate patients regarding kidney stone prevention, stent removals and physical recovery, such as after hip replacement surgery.
This article examines how well-written discharge materials can improve patient health by smoothing patient discharge, and helping self-management and health literacy.
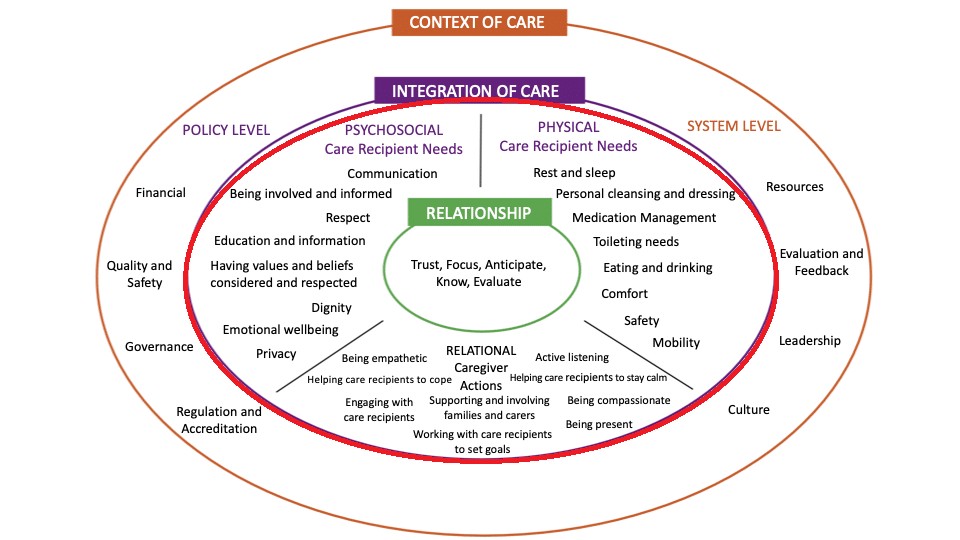
We examine this in the context of the integration of care domain (the red circle, below) — part of the fundamentals of care (FoC) framework.3

Student reflection
Observations from our clinical placements showed that written information enhanced condition management and health outcomes.
Across clinical specialities, patients who received written resources such as exercise sheets, intercostal chest drain care instructions, or crutch-use pamphlets demonstrated greater engagement and understanding.
They demonstrated confidence in self-care after discharge when reviewed during weekly follow-up clinics in the ward. In this context, we chose to explore the most effective forms of information-sharing for patients on discharge.
Background
Many patients face challenges in managing their health after hospital discharge due to a lack of clear information.1
While clinicians — nurses, doctors, and other health professionals — provide verbal education during hospitalisations, much can be forgotten without written information.

Patients struggle to retain discharge instructions, increasing risks of non-adherence to treatments, medication errors, overlooked adverse symptoms, and missed follow-ups.1
Written information, such as pamphlets, handouts and leaflets, can support verbal education by providing clear and accessible details on symptoms, surgical procedures, medications, recovery, and risks, using simple and understandable language.4
Holistic patient education reduces hospital readmissions, improves adherence to care after discharge, and decreases anxiety and stress.5
However, despite its benefits, some clinicians perceive written information as having little practical value, viewing it merely as a “nice thing to do for patients”.5
Benefits of written information
Involving patients in care planning and providing clearly-written information enhances their knowledge, supports informed decision-making, and strengthens health literacy, ultimately fostering better self-management and overall health.2, 5, 6

Patients with well-designed written information have reported increased knowledge, improved information recall and enhanced health literacy, which has led to better health management and reduced hospital readmissions.2,5,6
Additionally, a Canadian study identified that a quarter of patients who were not provided written information about symptom monitoring were readmitted within 43 days of discharge.7
Over half of patients who were not included in care planning and did not receive written information also had an increased risk of readmission.7
Therefore, active collaboration between nurses and patients is essential to reducing readmissions and improving health outcomes.
Limitations of written information
A key limitation involves language appropriateness.
‘While clinicians — nurses, doctors, and other health professionals — provide verbal education during hospitalisations, much can be forgotten.’
We observed that nurses faced challenges delivering safe and comprehensive discharge education due to limited interpreter availability and a lack of translated resources.
These barriers contributed to prolonged discharge wait times and made timely interpreter scheduling difficult.
This reflects New Zealand’s diverse population, where over one quarter of people speak languages other than English.8
The shortage of interpreters and translated resources hindered effective communication and patient education, compromising discharge safety and outcomes, which are essential to meeting physical care needs within the FoC framework.3,9
Delivery of complex information posed challenges. We noted that written resources were difficult for patients and their families to understand due to their complex format and information.

Ensuring that handouts were appropriate for individuals across all health literacy levels was a significant challenge.
Complex layouts, dense text, and excessive information increased the potential for information overload and hindered patient comprehension, particularly for those with cognitive impairments or anxiety.
These points highlight the importance of simple, clear, and visually accessible written materials.1,10
We also observed how limited resources impacted equitable access to information.
Not all health-care settings had available, up-to-date or culturally appropriate materials, which constrained patient access.
“Ensuring that handouts were appropriate for individuals across all health literacy levels was a significant challenge.”
Availability was further complicated by the current strict budget constraints within New Zealand’s health system, resulting in an inconsistent distribution of patient education resources nationwide.11,12
Furthermore, it has been noted5 that in many cases, written information was only provided at the patient’s request or at the discretion of the nurse, worsening inequities in information access.
These factors reflect the influence of the FoC framework’s context of care, specifically highlighting barriers in policy and systems in place.3
In the context of disability and diverse communication needs, written materials alone can be limiting if not adjusted appropriately to the patient’s preferences, accessibility and health literacy levels.
People with disabilities often experience barriers to health communication due to a lack of accessible formats and communication strategies.13
It can be harder to retain verbal instructions alone or to process written information without support.14 A recent study highlighted the importance of multiple approaches to enhance comprehension, demonstrating that relying solely on one mode of instruction significantly reduces recall among individuals with intellectual disabilities.15

For example, adults with mild intellectual disability recalled more information when learning involved vocal production, speaking or reading aloud, compared to when they only listened or read silently.15
Moreover, it has been demonstrated5 that a combination of written and standard verbal information also improved patients’ medication knowledge compared to providing verbal information alone.
The authors concluded that combining verbal and written communication significantly enhances patient understanding and self-management after discharge.
Despite these limitations, we identified some key strategies to improve the quality of the written information provided.
Simplified information pages
Researchers1 have evaluated the effectiveness of a more accessible simplified information page (SIP) in discharge instructions, which include the most crucial and often overlooked discharge information for patients, such as primary diagnosis, prescribed medications, potential adverse side effects, and important follow-up appointment dates.
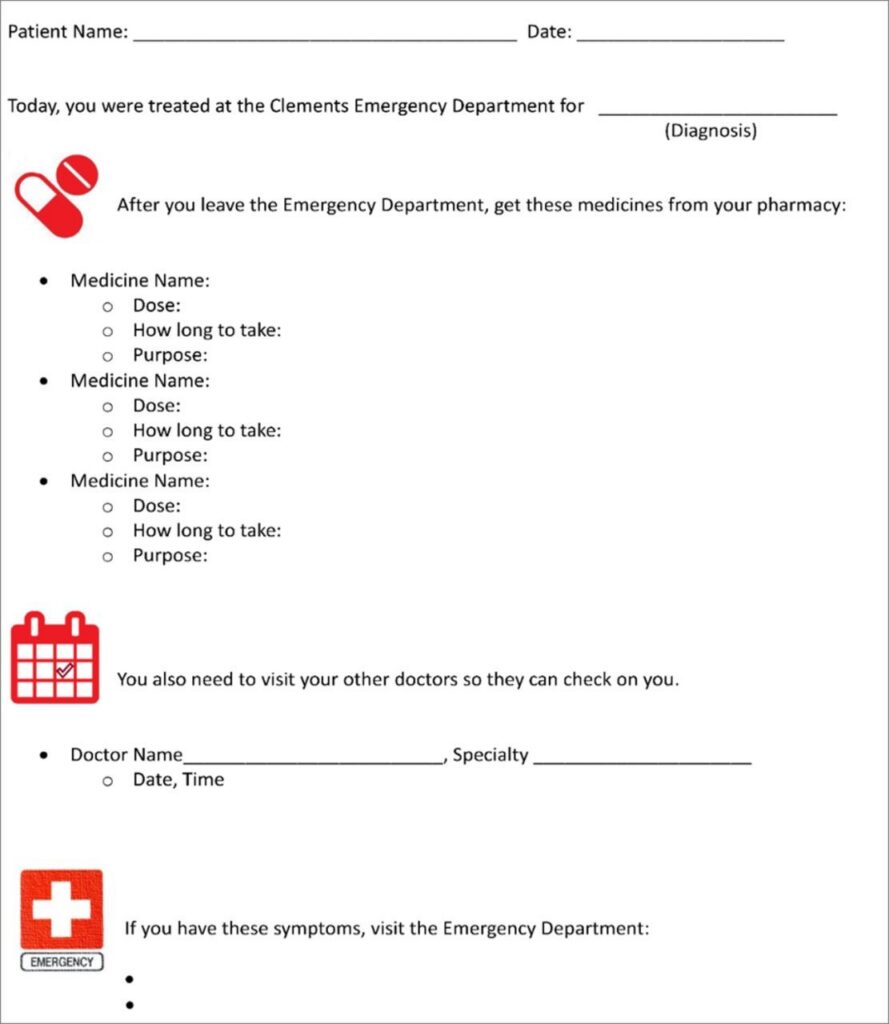
The SIP’s digestible information resulted in improved patient recall and understanding of critical discharge instructions, which reduced chances of readmission.1 An example is provided above in Figure 2.
Combining accessible and inclusive information modes
Multiple researchers2,5 have found that both verbal and written discharge instructions offer higher rates of accurate recall compared with those receiving only one form of communication — improving self-management.
We argue that utilising both verbal and written methods to educate patients, with or without disabilities, improves knowledge, understanding, and confidence in self-management, all of which are critical for effective post-discharge care.5
Recommendations for nursing practice and policy
Written content should use minimal medical jargon and be available in multiple languages to support understanding across all health literacy levels, especially for individuals whose English is not their first language.6
Organisational support is needed to provide discharge materials in multiple languages, especially for common non-English languages in the local community.
We also recommend policies that ensure timely access to interpreters to enhance verbal communication alongside written translations during the discharge process. This will enable nurses to deliver safer education, reduce communication barriers, and improve patient understanding and safety.9
Meeting patients’ education and information needs through accessible language, improving understanding and increasing satisfaction with the education provided addresses psychosocial needs in line with the FoC framework.3,16
Additionally, enhancing financial support through system-level policies would enable all healthcare settings to afford the production and distribution of high-quality written information promoting consistent and equitable access to patient education nationwide.3
We recommend that nurses advocate for the routine use of written materials as a standard part of their discharge education routine to help patients receive accurate information.
Personalised educational approach
Greater patient engagement and confidence were observed in our clinical placements when nurses took time to review discharge information, simplifying the language and using drawings and annotations to aid patients’ understanding.
We encourage nurses to use plain, everyday language when providing verbal and written education, avoiding medical jargon.
We also recommend annotating handouts to highlight key information and encouraging patients to ask questions to confirm their understanding.
Local and government organisations, such as Healthify NZ17, Medsafe18, MIMS (Monthly Index of Medical Specialities) New Zealand19, and resources available within Health Information Platform for Practitioners Online already offer accessible, patient-friendly health information.
Nurses should utilise these reliable resources to reduce the time spent simplifying complex handout information.
In the spirit of the integration of the care domain in the FoC framework, engaging patients in the design of handouts can further enhance their effectiveness by seeking patient feedback on language, layout and illustrations to ensure materials are understandable and aligned with patient priorities.21, 3
A personalised, patient-centred approach to education may improve patient satisfaction, understanding, and treatment adherence, highlighting the importance of tailoring resources to individual needs rather than relying solely on standardised formats.22
‘We encourage nurses to use plain, everyday language when providing verbal and written education, avoiding medical jargon.’
Multidisciplinary team collaboration
We recommend that nurses actively engage in multidisciplinary team (MDT) collaboration to ensure accurate, timely and accessible information is provided on discharge, working alongside the likes of pharmacists, interpreters, cultural support, and social workers.
Collaboration helps ensure that patients receive clear, culturally appropriate and understandable information about their care, medications and support.
This should also include proactively referring patients with disabilities to appropriate support services to ensure a safe and informed discharge process.
Research23 has found that effective discharge information and planning are facilitated by communication among patients, families, and MDT members, leading to shared expectations and improved patient outcomes.
Collaboration supports effective communication, continuity of care across different disciplines and improves patient outcomes.

Conclusion
Obstacles to using written information effectively include language barriers, poor pamphlet design, and limited resources.
These factors can lead to inadequate patient education, resulting in low health literacy, poor treatment adherence, and ineffective management of the condition.
Therefore, nurses need to integrate patient-centred education at discharge, using clear verbal and written information to enhance understanding, particularly for individuals with intellectual disabilities.
Organisational support is vital to ensure discharge materials are available in multiple languages and that policies facilitate timely access to interpreters, promoting equitable and effective patient education.
These approaches align with the FoC framework by strengthening both the relational domain, through effective communication and therapeutic partnerships, and the contextual domain, through supportive systems and policies that enable consistent, equitable care.3
Overall, these bedside and system-level recommendations provide a practical pathway to safer, more person-centred transitions from hospital to home.
Claire Samuel, Sieun Kim, Francine Llanillo, Lorenzo Marcelo, Kiran Karaka and Chenhao Yang are final-year bachelor of nursing students at the University of Auckland. They began working on this article during their second year of study and are due to graduate this year. Kim Ward is a senior lecturer at the School of Nursing at the University of Auckland.
References
- DeSai, C., Janowiak, K., Secheli, B., Phelps, E., McDonald, S., Reed, G., & Blomkalns, A. (2021). Empowering patients: Simplifying discharge instructions. BMJ Open Quality.
- Hoek, A. E., Anker, S. C. P., van Beeck, E. F., Burdorf, A., Rood, P. P. M., & Haagsma, J. A. (2020). Patient discharge instructions in the emergency department and their effects on comprehension and recall of discharge instructions: A systematic review and meta-analysis. Annals of Emergency Medicine, 75(3), 435–444.
- Kitson, A., Conroy, T., Kuluski, K., Locock, L & Lyons, R. (2013). Reclaiming and redefining the Fundamentals of Care: Nursing’s response to meeting patients’ basic human needs, School of Nursing, the University of Adelaide.
- Perri, S., Argo, L., Kuang, J., Bui, D., Hill, B., Bray, B., Treitler-Zeng, Q. (2016). A picture’s meaning: The design and evaluation of pictographs illustrating patient discharge instructions. Journal of Communication in Healthcare, 8(4), 335–349.
- Johnson, A., Sandford, J., & Tyndall, J. (2003). Written and verbal information versus verbal information only for patients being discharged from acute hospital settings to home. Cochrane Database of Systematic Reviews, 2003(4).
- Rameshkumar, T., Haputhanthrige, I. U., Misbahunnisa, M. Y., & Galappatthy, P. (2022). Patients’ knowledge about medicines improves when provided with written compared to verbal information in their native language. 17(10).
- Kemp, K. A., Quan, H., & Santana, M. J. (2017). Lack of patient involvement in care decisions and not receiving written discharge instructions are associated with unplanned readmissions up to one year. Patient Experience Journal, 4(2), 4.
- Infometrics New Zealand. (2023). Regional Economic Profile | Auckland | Census | Languages spoken. Infometrics. Retrieved May 14, 2025.
- Shamsi, H. A., Almutairi, A. G., Mashrafi, S. A., & Kalbani, T. A. (2020). Implications of Language Barriers for Healthcare: A Systematic Review. Oman Medical Journal, 35(2).
- Khaleel, I., Wimmer, B. C., Peterson, G. M., Zaidi, S. T. R., Roehrer, E., Cummings, E., & Lee, K. (2020). Health information overload among health consumers: A scoping review. Patient Education and Counselling, 103(1), 15-32.
- Goodyear-Smith, F., & Ashton, T. (2019). New Zealand health system: universalism struggles with persisting inequities. Lancet (London, England), 394(10196), 432–442.
- Ministry of Health. (2024, November 13). An overview of Vote Health funding for the health system in Budget 2024.
- Krahn, G. L., Walker, D. K., & Correa-De-Araujo, R. (2015). Persons with disabilities as an unrecognised health disparity population. American journal of public health.
- Barrington, M., Fisher, K. R., Harris-Roxas, B., Spooner, C., Trollor, J. N., & Weise, J. (2025). Access to healthcare for people with intellectual disability: a scoping review. Scandinavian Journal of Public Health.
- Icht, M., Ben-David, N., & Mama, Y. (2021). Using Vocal Production to Improve Long-Term Verbal Memory in Adults with Intellectual Disability. Behavior Modification, 45(5), 715–739.
- Oliveira, V. C., Refshauge, K. M., Ferreira, M. L., Pinto, R. Z., Beckenkamp, P. R., Negrao Filho, R. F., & Ferreira, P. H. (2012). Communication that values patient autonomy is associated with satisfaction with care: a systematic review. Journal of physiotherapy, 58(4), 215-229.
- Healthify NZ.
- Medsafe. New Zealand Medicines and Medical Devices Safety Authority.
- MIMS New Zealand.
- Pratt, M., & Searles, G. E. (2017). Using Visual Aids to Enhance Physician-Patient Discussions and Increase Health Literacy. Journal of Cutaneous Medicine and Surgery, 21(6), 497–501.
- Fong, S., Tan, A., Czupryn, J., & Oswald, A. (2019). Patient-centred education: How do learners’ perceptions change as they experience clinical training? Advances in Health Sciences Education, 24, 15-32.
- Gledhill, K., Bucknall, T. K., Lannin, N. A., & Hanna, L. (2023). The role of collaborative decision-making in discharge planning: Perspectives from patients, family members and health professionals. Journal of Clinical Nursing, 32(19-20), 7519–7529.