
|
ABSTRACTBackground: Oral care is a fundamental part of nursing care, especially for care-dependent older adults, yet it remains one of the most neglected nursing interventions. This is largely due to the lack of standard nursing oral care protocols, effective training and awareness of the benefits for older adults. Aim: The aim of this research will be to establish evidence-based oral care guidelines, using interprofessional collaboration and education, with the aim of improving nursing oral care practice. We also plan to pilot these guidelines with community nursing staff to determine their effectiveness and acceptability. Method: The proposed research will use mixed methods and participatory action with co-design, underpinned by interprofessional collaboration and education, to develop evidence-based nursing oral care guidelines, training modules and supporting resources, and to evaluate effectiveness among community nursing staff. Conclusion: The oral care guidelines, training resources and evaluation approaches we will co-develop will enable community nursing staff to develop their own, locally-approved evidence-based nursing oral health-care protocols. Thus, this study will be a stepping stone in the promotion of nurse-led oral care and normalising of sustainable oral care practice, with the goal of promoting older adults’ oral health and overall health and wellbeing. |
|||||||||||||||
KEYWORDSoral care, nursing, care-dependent, older adults, protocols, interprofessional collaboration and education |
||||||||||||||||
 Keiko Oda
Keiko Oda Noor Nazahiah Bakri
Noor Nazahiah Bakri Sarah Majeed
Sarah Majeed Catherine Anna Ferguson
Catherine Anna Ferguson Shennae Bartlett
Shennae Bartlett Rachel Holden
Rachel Holden W Murray Thomson
W Murray Thomson John Parsons
John Parsons Michal Boyd
Michal Boyd Moira Smith
Moira SmithINTRODUCTION
LITTLE IS KNOWN ABOUT oral nursing care practice which supports care-dependent older adults’ oral health, especially those ageing in their own homes, owing to a lack of interprofessional collaboration, and nursing oral care guidelines. The lack of nursing oral care for care-dependent older adults is an ongoing problem in aged care. This study protocol will guide the establishment and implementation of a co-developed set of guidelines, training modules and resources, and evaluation approaches based on IPC/IPE (interprofessional collaboration and education) that will provide on-site, hands-on oral health training and support for nursing oral care practice.
This paper presents a research protocol for a study that aims to:
(i) develop a guideline for conducting a nurse-led oral care assessment and developing a support or care plan for care-dependent older adults, and develop associated training and other resources to support the guideline’s implementation, utilising interprofessional collaboration and education, and co-design; and
(ii) improve nurses’ knowledge, confidence and self-efficacy in oral nursing care, through the guideline and training.
The study aims to answer the following research questions:
(i) whether an oral care guideline can improve nursing oral practice by enhancing knowledge and confidence; and
(ii) whether an oral care guideline can facilitate the normalisation of daily nursing oral care practice.
BACKGROUND
Oral care is a fundamental part of nursing practice (Aagaard et al, 2020; Gibney et al, 2019; Hatchett, 2021; Jablonski et al, 2018; Oda, 2017). Nursing oral care involves oral health education and promotion, supporting or performing oral hygiene procedures, assessing patients for oral diseases and disease risk, and treatment of diseases of the oral mucosa, lips, teeth, gums, and tongue (Kilkenny, 2019). The aim of oral care is to help patients maintain a comfortable and clean mouth and maintain oral functions, including eating, speaking, and smiling (Maruoka et al, 2022).
Oral care is especially important for care-dependent older adults – those being supported to live in the community or those who live in aged residential care (ARC) facilities (Hatchett, 2021; Jablonski et al, 2018). Their complex and high health-care needs place them at substantial risk of oral disease, oral deconditioning and sub-optimal oral health, more so than their independent peers. Many care-dependent older adults have difficulty accessing oral health care services owing to the high cost of dental treatment, and physical and cognitive challenges. In many developed countries, including New Zealand, care-dependent older adults’ routine dental care is generally not publicly-funded, subsidised or provided at their place of residence (Schluter, 2021; Smith, 2010).
Nurses have a key role in maintaining good oral hygiene and function among the care-dependent older adults they care for. Nursing oral care can improve oral health-related quality of life, and reduce the risk of oral disease and incidence of aspiration pneumonia and deconditioning, along with subsequent hospital admissions (Oda et al, 2021). In residential settings, nurses play a large part in determining the nature of the support or care that care-dependent older people receive. The support or care plans nurses develop, and that are subsequently implemented by support or care workers, are typically informed by clinical and social information gathered from a range of sources.
Despite its importance, oral care remains one of the most neglected nursing interventions, with care-dependent older adults unlikely to regularly receive basic nursing oral care at their place of residence (Gibney et al, 2019; Schluter et al, 2021; Thompson et al, 2019). Their oral health is rarely assessed as part of the support or care planning process. Consequently, nursing oral care directives seldom feature in older adults’ support or care plans. This gap is largely a consequence of a lack of standard nursing oral care guidelines, training and skills; a lack of awareness among nurses of the benefits of nursing oral care for care-dependent older adults; and a lack of formal oral care policies and procedures in community health-care support and ARC systems (Gibney et al, 2019; Jablonski et al, 2018; Woon, 2020). Moreover, there is little research on nurse-led oral care assessments of care-dependent older adults (Manchery, et al, 2020), especially in New Zealand, to inform change.
Providing oral nursing care for care-dependent older people in their place of residence, guided by a set of guidelines, and as a regular feature of assessment and planning systems, would prevent oral disease progression and its sequelae. It would also provide a process for referral to specialist care when required. In turn, these actions would improve older people’s overall health and wellbeing, and reduce the subsequent burdens on them, their families, whānau and carers, and the health system.
International guidelines recommend establishing standardised oral care guidelines for care-dependent older adults (NICE, 2016; SA Health, 2008; Zimmerman et al, 2020). The guidelines should be person-centred, evidence-based and delivered by a multi-disciplinary team that includes nurses. The purpose of the guidelines is to improve oral hygiene, prevent oral disease and aspiration pneumonia, enhance dysphagia rehabilitation, and improve overall quality of life (Maeda & Akagi, 2014; Oda, 2017; Quinn et al, 2014; Woon, 2020). Evidence demonstrates person-centred care is critical in the provision of nursing oral care (Jablonski et al, 2018; Zimmerman et al, 2020). For nurses, oral care guidelines need to be relevant to nursing practice, and achievable within nurses’ capacity and capability. Three key factors for improving nursing oral care practice are: interprofessional collaboration and education, onsite nursing oral care training, and integration of contextual knowledge and competencies of all stakeholders in oral care provision (Aagaard et al, 2020; Keboa et al, 2019; Lewis et al, 2019; Niesten et al, 2020). Interprofessional collaboration and education helps overcome some of the barriers to nursing oral care by minimising disciplinary silos and hierarchical power dynamics that can occur in an interdisciplinary team (Brocklehurst et al, 2021; Niesten et al, 2020), improving nurses’ oral care knowledge and practice skills, and enhancing their capacity to successfully deliver oral care.
METHOD
This study is a key component of a broad programme of research projects that are investigating how to improve the oral health-related quality of life and wellbeing of care-dependent older New Zealanders, and in turn contribute to their overall health and wellbeing. The programme of research aims to:
(i) raise oral health knowledge, and skill and confidence in providing preventive oral health care among staff, and clients or residents, and their family and whānau, and
(ii) determine feasible, acceptable and sustainable preventive oral health care policies and procedures in supported care and ARC facilities to ensure an acceptable standard of oral health and wellbeing among clients and residents.
Ultimately, the research programme’s goal is for preventive oral health care policies and procedures to be embedded within community-based health-care support and ARC in New Zealand. This paper presents the research protocol for the nurse-led assessment part of the research programme.
In late 2020, a collaboration was formed among researchers from the University of Auckland’s School of Nursing and Public Health, the Department of Public Health at the University of Otago, Wellington, and the Faculty of Dentistry at the University of Otago. The interprofessional research team comprises a registered nurse (KO), two oral health therapists (SM and RH), and dentists and oral health academics (NNB, MS, SB, CAF, WMT). Members of the research team had established prior collaborative relationships with a leading community health-care support provider and an ARC provider; both providers sought to collaborate further with the research team on this study. The research team will work with staff and clients from the community provider, and two ARC facilities (one urban, one provincial), in the lower half of the North Island of New Zealand.
Study design
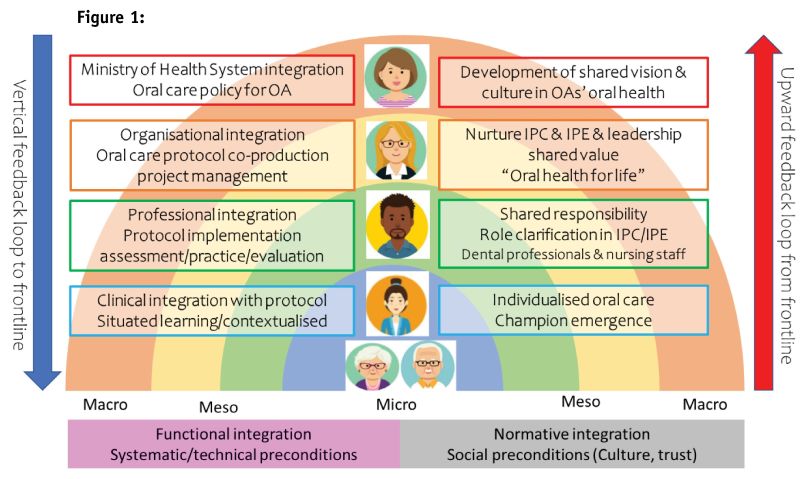
This study will use a mixed-methods approach. To enhance the active participation of all stakeholders, it uses participatory action research with co-design. Co-design is an approach to working with people that enables the connection of ideas, skills and resources to experiment with new ideas and strategies for research (Zamenopoulos & Alexiou, 2018). To clarify the roles of all stakeholders, including individual researchers within the team, systems mapping (Niesten et al, 2020) was undertaken to navigate the project with all stakeholders. The system map (see Figure 1, below) illustrates the roles at the policy development (macro), organisational-interprofessional (meso), and individual-clinical (micro) hierarchical levels with the aspiration of upwards feedback to policymakers.
The study comprises two stages:
(I) the development of a nurse-led oral care assessment and planning guideline, and
(II) the development and delivery of nurse and support/care worker oral care and assessment training.
Both stages include measures to evaluate them for effectiveness and acceptability.
Participant recruitment
Inclusion criteria
Those eligible to participate in this study include: nurses and support/care workers who plan and support/provide health care for clients/residents; clinical or training managers, employed by either of the provider collaborators; and clients/residents of the provider collaborator organisations.
Exclusion criteria
Locum nursing staff will be excluded.
Participants will be recruited purposively. The study will be introduced to the providers’ staff at a time convenient to the organisations’ management teams. Eligible staff interested in participating will advise their managers and will be contacted by the research team to provide them with more information and gain consent. All meetings will be made in arrangement with participants and management and held at times and locations convenient to them. Up to eight nurses (four from the community provider and four from the ARC providers) will be recruited.
Stage I: Development of nursing oral care guidelines
Informed by a review of the current literature and recommendations of leading health organisations, the interprofessional team will develop an initial draft of a person-centred, oral health-care assessment and planning tool for use by nurses. The tool will form the basis of the guidelines for nurses to conduct oral care assessments and develop support/care planning. It is anticipated that by using the oral care nursing guidelines, nurses will be able to identify clients’ or residents’ clinical oral health-care needs (“normative needs”) and their oral health-care preferences (“felt needs”). Subsequently the nurses will be able to develop individualised oral care recommendations for inclusion in clients’ or residents’ overall support or care plans (for implementation by care/support workers), and regularly monitor clients’ or residents’ oral health (Mc et al, 2022).
The tool is informed by the Oral Health Assessment Tool (OHAT) developed by Chalmers et al (2005). OHAT is a validated tool originally designed for use by non-oral health professionals to assess the oral health of older adults with dementia. The assessment comprises eight components: lips, tongue, oral mucosa, saliva, teeth, dentures, oral cleanliness and pain. During the study’s formative stages, the research team identified gaps in the OHAT, primarily the absence of an assessment of felt needs. The tool also lacked assessment accuracy, and included minimal individualised oral care planning, minimal capacity to ensure its implementation and measure its effectiveness, and no mechanism for referral to health professionals (Chalmers et al, 2005; Jablonski et al, 2018). The amended tool will likely include mechanisms to monitor changes in clients’ oral health over time, and to enable referral pathways and person-centred care.
To support the tool, information resources will be developed. They will include referral pathways to dental services (in the form of flowcharts), a list of dental services available in the region, information on how to apply for publicly-available financial assistance, and infographics on the care of natural teeth and dentures, and approaches for delivering dry mouth care. In addition to use by nurses, the resources (with exception of the referral pathway) will also be intended for use by clients/residents, family and whānau, and care/support workers.
Stage II: Development and delivery of oral care and assessment training
To support the guideline and its application in nursing practice, an initial draft of an accompanying training module for nurses will be developed by the research team. Informed by international guidelines, existing training programmes and the scientific literature, the module will comprise two theoretical, didactic sessions. The first session will inform participants of the importance of oral health and oral health care, and specific information on the care for care-dependent older adults will be included. This session is intended for nurses, other clinical staff (such as clinical managers and trainers) and support/care workers, and will be no more than 90 minutes in duration, including time for questions and discussion. Information resources will be distributed among participants at this session.
The development of the training modules and the accompanying resources will be based on the principles of participatory action research and co-design. Participatory action research with co-design is suitable for community-based nursing oral care quality projects, as nursing staff are practising individualised care in complex home-based environments by sharing power with vulnerable older adults (Stark, 2022). Thus, the researchers and participants are interdependent, and the researchers are aware of their role as facilitators to bring change in practice. This helps to eliminate professional jargon, cuts across discipline silos, connects people, and promotes participation to address a common research goal in a meaningful way for participants. Before the resources are disseminated to the study participants, feedback will be sought from a range of people with knowledge of the care of care-dependent older adults, such as older adults, those working in caregiver roles, oral health professionals, nurse educators and nurses, to ensure that the use of language, the amount and level of information, the visual design and the presentation style are appropriate. Following initial development and prior to delivery, the tool, and the content and delivery plan for the training sessions, will then be shared and discussed with the management teams from both collaborating providers. The research team will gather their feedback on the likely acceptability and feasibility of the intended content and delivery to their nursing staff, and alignment with the organisations’ usual training practices and procedures. All material will be amended in accordance with the feedback.
The second training session is intended for nurses and will provide information specifically on oral health-care assessment and planning, and the use of the tool. In this session, the participants will receive practical, hands-on training on conducting oral health assessments and subsequently developing support or care plans, with the support of the team’s oral health practitioners. Assessments will initially be conducted in-class with research team members acting as “clients/residents”. This will be followed by in-field sessions with clients/residents (that is, in their place of residence), with the team’s oral health practitioners in attendance to support the participating nurses. At the conclusion of the in-class session, the participating nurses will be asked to identify and approach clients/residents who they think would be interested in participating in a research project about oral health. They will then describe the study to those clients or residents and gauge their interest in participating, and provide study information sheets and consent forms. The nurses will seek permission from interested clients or residents for their contact details to be passed onto the study team to arrange consent and provide further information. Up to 10 clients or residents will be recruited. Times convenient to consenting clients/residents and nurses for the in-field assessments will be arranged. Following their assessment, the participating clients/residents will be interviewed to gather their views on having their oral health assessed and included in their support/care plan, and suggestions for improvement.
Evaluation
Data collection and analysis
To evaluate the efficacy of the training modules and assessment sessions, the research team will administer questionnaires electronically (Qualtrics) before and after the training sessions. The questionnaires will gather information so that changes in in participants’ knowledge, attitude, and confidence in oral care practice can be measured. The questionnaire will comprise 37 items, informed by previous studies (Edwards et al, 2021; Frenkel et al, 2002; Haresaku et al, 2020; Wretman et al, 2020). The knowledge section will comprise 19 items on oral health, seeking “yes/no/don’t know” responses; there will also be 13 confidence and self-efficacy items using a 5-point Likert scale; and five items on the usability of the OHAT scale, also seeking Likert responses. (See Appendix 1, p56-57.) Data will be analysed descriptively using t-test and Pearson’s correlation test by SPSS version 27.
At the conclusion of the training sessions, two focus groups (one from each of the provider collaborators) will be conducted with the participating nurses (up to eight). Guided by a semi-structured interview schedule, the focus group discussion will gather the nurses’ feedback on the relevance and delivery of the training module, the acceptability of undertaking an oral care assessment on clients/residents and the feasibility of the tool and its incorporation into their organisations’ existing care and care-planning systems. The nurses will also be asked for their suggestions on improvements in the training and the tool. Qualitative data will be analysed thematically to identify oral care barriers and facilitators, and recommendations will be developed for improving the visibility of oral care for nursing staff and clients.
The appropriate level of ethical approval will be sought before data collection starts.
DISCUSSION
Nursing oral care for care-dependent older adults is little practised, largely owing to a lack of training, guidelines and awareness of its importance for older adults, their families and carers, and the health system. There is also a lack of evidence to inform action to address this issue, particularly in New Zealand. The research protocol presented in this paper describes a study that aims to initiate changes in nursing practice, so as to better support care-dependent older adults’ health and wellbeing. Through interprofessional collaboration and education, involving nurses and oral health professionals, and a co-design approach, the study aims to develop evidence-based nursing oral care guidelines, and supporting training modules and resources. These will then be evaluated for feasibility and acceptability among nurses and care-dependent older adults they care for. The approaches used in this study are expected to result in a more practical, equitable and sustainable way to meet the oral care needs of care-dependent older adults than through a conventional hierarchical system (Brocklehurst et al, 2021).
The interprofessional collaboration and education will create an opportunity to exchange knowledge and expertise between nursing and oral health-care professionals, and to co-produce clinical knowledge for the delivery of oral nursing care for care-dependent older adults (Buck et al, 2021; Cole, 2020). For example, nursing staff learning from oral health professionals will likely enhance their clinical assessment skills so they can identify the oral conditions that can trigger deconditioning. Oral health is typically isolated from other aspects of health care practice. This study will allow oral-health professionals to learn from nursing staff about gerontological nursing practice and how best to integrate oral care into it (Keboa et al, 2019). Moreover, the onsite support of nursing oral care practice by oral health professionals will likely generate the contextual knowledge required to address clients’ daily oral care needs and oral care provision (Aagaard et al, 2020). Consequently, nursing oral care training based on interprofessional collaboration and education will likely be a key factor in ensuring nursing oral care becomes a core competency in gerontological nursing.
At a local organisational level, interprofessional collaboration and education will likely allow for the implementation of train-the-trainer approaches to facilitate sustainable in-house training of nursing and support worker staff (Buck et al, 2021; Truant et al, 2017). Train-the-trainer approaches, based on interprofessional collaboration and education, can enhance leadership among nursing staff and increase the capacity and confidence of nursing oral care assessments. Upward feedback on the barriers and facilitators for oral care provision from frontline nursing staff to decision and policymakers at all organisational levels is an important component of achieving effective changes to oral health care policy for care-dependent older adults (Aagaard et al, 2020; Niesten et al, 2020). Ultimately, the aspiration is to establish a bidirectional feedback system that will enable the provision of ongoing support for nursing staff to deliver oral nursing care for care-dependent older adults in a way that is sustainable and normalised into their overall care practice (see Figure 1, above).
This study will be one of the first to address nursing oral care practice of care-dependent older adults in the community and to use interprofessional collaboration and education to do so. The guidelines that will be developed will be based on evidence, and international guidelines and recommendations, and the processes developed will be informed by “real-world” information. Although care assessment and planning processes may differ among providers, the tools, resources and processes developed in this study are likely to be useful for other providers, or to be amended to meet their specific needs and align with their processes.
A range of health disciplines have a role in providing comprehensive oral health care for older adults. While this study’s interprofessional collaboration team will provide varying perspectives on, and understanding of, oral health care for care-dependent older adults, the absence of other health professionals, such as dietitians and speech-language therapists, may be a limitation. Nevertheless, the team intends to develop a local and relevant oral nursing care guideline and training module, that includes an assessment of felt needs, and extends and contemporises the OHAT, ensuring a comprehensive approach to care-dependent older adults’ oral health care. We think the guidelines and training module will likely be suitable for use with ARC residents, providing consistency in oral health-care assessment and planning across the levels of aged care (Takeda et al, 2020).
CONCLUSIONS
This study protocol outlines a critical step towards improving nursing knowledge, practice and awareness of the importance of oral care for care-dependent older adults. The study will do so through co-development of an evidence-based set of guidelines, training resources and evaluation approaches using interprofessional collaboration and education. By helping to break down health-care delivery siloes and hierarchies, the outcomes of this study will likely enhance nursing leadership, and lead to sustainable oral health-care for our older population.
ACKNOWLEDGEMENT
The authors would like to thank Professor Fredrick Wright of the Melbourne Dental School for his support for the development of these oral health guidelines.
REFERENCES
Aagaard, K., Meléndez-Torres, G. J., & Overgaard, C. (2020). Improving oral health in nursing home residents: A process evaluation of a shared oral care intervention. Journal of Clinical Nursing, 29(17/18), 3392-3402.
Brocklehurst, P. R., Baker, S. R., & Langley, J. (2021). Context and the evidence-based paradigm: The potential for participatory research and systems thinking in oral health. Community Dentistry and Oral Epidemiology, 49(1), 1-9. https://doi.org/10.1111/cdoe.12570
Buck, H. G., Boltz, M., Madrigal, C., Eshraghi, K., & Kolanowski, A. M. (2021). Using Appreciative Inquiry to Optimize a Person-Centered Care Training Program for Clinical Champions in Rural Critical Access Hospitals. Journal of Gerontological Nursing, 47(8), 7-12.
Chalmers, J. M., King, P. L., Spencer, A. J., Wright, F. A., & Carter, K. D. (2005). The oral health assessment tool – validity and reliability. Australian Dental Journal, 50(3), 191-199.
Cole, E. (2020). A nurse champion of oral care in community services. Primary Health Care, 30(6), 13-15.
Edwards, C. B., Randall, C. L., & McNeil, D. W. (2021). Development and Validation of the Oral Health Values Scale. Community Dentistry and Oral Epidemiology, 49(5), 454-463.
Frenkel, H., Harvey, I., & Needs, K. (2002). Oral health care education and its effect on caregivers’ knowledge and attitudes: a randomised controlled trial. Community Dentistry and Oral Epidemiology, 30(2), 91-100.
Gibney, J. M., Wright, F. A., D’Souza, M., & Naganathan, V. (2019). Improving the oral health of older people in hospital. Australasian Journal on Ageing, 38(1), 33-38.
Haresaku, S., Miyoshi, M., Kubota, K., Aoki, H., Kajiwara, E., Monji, M., & Naito, T. (2020). Effect of interprofessional education on oral assessment performance of nursing students. Clinical and Experimental Dental Research, 6(1), 51-58.
Hatchett, R. (2021, Sept 20). How to undertake effective mouth care and oral assessments. Nursing Standard.
Jablonski, R. A., Kolanowski, A. M., Azuero, A., Winstead, V., Jones-Townsend, C., & Geisinger, M. L. (2018). Randomised clinical trial: Efficacy of strategies to provide oral hygiene activities to nursing home residents with dementia who resist mouth care. Gerodontology, 35(4), 365-375.
Keboa, M., Beaudin, A., Cyr, J., Decoste, J., Power, F., Hovey, R., LaFrance, L., Ouellet, D., Wiseman, M., & Macdonald, M. E. (2019). Dentistry and nursing working together to improve oral health care in a long-term care facility. Geriatric Nursing, 40(2), 197-204.
Kilkenny, N. (2019). Oral care in adults. British Journal of Nursing, 28(16), 1054-1055.
Lewis, A., Harvey, G., Hogan, M., & Kitson, A. (2019). Can oral healthcare for older people be embedded into routine community aged care practice? A realist evaluation using normalisation process theory. International Journal of Nursing Studies, 94, 32-41.
Maeda, K., & Akagi, J. (2014). Oral care may reduce pneumonia in the tube-fed elderly: a preliminary study. Dysphagia, 29(5), 616-621.
Manchery, N., Subbiah, G. K., Nagappan, N., & Premnath, P. (2020). Are oral health education for carers effective in the oral hygiene management of elderly with dementia? A systematic review. Dental Research Journal (Isfahan), 17(1), 1-9.
Maruoka, Y., Michiwaki, Y., Sekiya, H., Kurasawa, Y., & Natsume, N. (2022). What does oral care mean to society? Bioscience Trends, 16(1), 7-19.
Mc, G. C., Suen, R. P., Mc, K. G., Moore, C., & Wong, M. C. (2022). Oral Health and Successful Ageing – The PROS and dPROS: A Scoping Review. Journal of Evidence Based Dental Practice, 22(3), 101714.
National Institute for Health and Care Excellence (NICE). (2016). Oral health for adults in care homes (NG48).
Niesten, D., Gerritsen, A. E., & Leve, V. (2020). Barriers and facilitators to integrate oral health care for older adults in general (basic) care in East Netherlands. Part 1: Normative integration. Gerodontology, 38(2), 154-165.
Oda, K. (2017). Oral health vital for hospitalised elderly: ensuring the elderly receive oral care while in hospital can play an important part in preventing functional decline. Kai Tiaki New Zealand, 23(10), 14-17.
Oda, K., Montayre, J., Parsons, J., & Boyd, M. (2021). Oral Care in Hospital Settings: Breaking the Vicious Circle of Older Adult Deconditioning. Journal of Gerontological Nursing, 47(6), 7-12.
Quinn, B., Baker, D. L., Cohen, S., Stewart, J. L., Lima, C. A., & Parise, C. (2014). Basic nursing care to prevent nonventilator hospital-acquired pneumonia. Journal of Nursing Scholarship, 46(1), 11-19.
SA Health. (2008). Better Oral Health in Residential Care: Professional Portfolio. Government of South Australia.
Schluter, P. J., Askew, D. A., McKelvey, V. A., Jamieson, H. A., & Lee, M. (2021). Oral Health Among Older Adults With Complex Needs Living in the Community and in Aged Residential Care Facilities within New Zealand. Journal of the American Medical Directors Association, 22(6), 1177-1183.
Smith, M. B. (2010). Oral health and well-being of older adults in residential care facilities: issues for public health policy. New Zealand Dental Journal, 106(2), 67-73.
Stark, P., McKenna, G., Wilson, C. B., Tsakos, G., Brocklehurst, P., Lappin, C., Quinn, B., & Mitchell, G. (2022). Interventions supporting community nurses in the provision of oral healthcare to people living at home: a scoping review. BMC Nursing, 21(1), 269.
Thompson, L., Jiang, T., Savageau, J. A., Silk, H., & Riedy, C. A. (2019). An Assessment of Oral Health Training Among Geriatric Fellowship Programs: A National Survey. Journal of the American Geriatrics Society, 67(5), 1079-1084.
Truant, T. L., Green, E., de Calvo, L. E. A., McCarthy, S. M., MacDonald, D., Patel, K., Stewart, J., Brunelli, M., Cullen, C., Estrada de Ellis, S., Nunes, L., & Salles, P. (2017). Enhancing Nurses’ Oral Therapy Practice in 4 Latin American Countries: A Collaborative and Participatory Approach. Cancer Nursing, 40(6), E49-E59.
Woon, C. (2020). Improving oral care for hospitalised patients: choosing appropriate products. British Journal of Nursing, 29(9), 520-525.
Wretman, C. J., Zimmerman, S., Ward, K., & Sloane, P. D. (2020). Measuring Self-Efficacy and Attitudes for Providing Mouth Care in Nursing Homes. Journal of the American Medical Directors Association, 21(9), 1316-1321.
Zamenopoulos, T., & Alexiou, K. (2018). Co-design as collaborative research. Bristol University/AHRC Connected Communities Programme.
Zimmerman, S., Sloane, P. D., Ward, K., Wretman, C. J., Stearns, S. C., Poole, P., & Preisser, J. S. (2020). Effectiveness of a Mouth Care Program Provided by Nursing Home Staff vs Standard Care on Reducing Pneumonia Incidence: A Cluster Randomized Trial. JAMA Network Open, 3(6), e204321.
APPENDIX 1
Please respond to the following 19 oral health statements with YES/NO/DON’T KNOW
1) Dentures should be taken out at night.
2) Denture cleaning solutions can clean dentures without you needing to brush them as well.
3) Dentures should be rinsed after every meal.
4) People without any natural teeth only need a dental check-up when they have a problem.
5) If people have a gum infection under their dentures, they also experience discomfort.
6) A dirty denture is unlikely to cause disease in the mouth
7) Wearing a denture increases the risk of mouth infection.
8) A toothbrush with soft bristles is better than one with hard bristles for cleaning teeth.
9) A smaller-headed toothbrush is better at cleaning teeth than one with a large head.
10) Toothbrushes should be changed every three months or when the bristles are worn.
11) A strip of toothpaste should be applied across the top surface of the toothbrush.
12) Older people’s teeth are less likely to become decayed than younger people’s teeth.
13) Brushing teeth will also improve the condition of the gum.
14) If people have a lot of sugary food and drink, their teeth are more likely to decay.
15) Cleaning teeth with a wet gauze or a clean towel is a good alternative to a toothbrush for cleaning teeth.
16) People who have dry mouth will tend to get less decay.
17) Even if the gums around the teeth are inflamed or bleeding, they do not usually cause any pain.
18) For health and safety reasons, you should wear protective gloves when cleaning older people’s teeth or
denture.
19) Once gum disease has started. it is almost impossible to stop it.
Please respond to the following 18 statements with 1. Strongly agree, 2. Somewhat agree, 3. Neither agree nor disagree, 4. Somewhat disagree, 5. Strongly disagree.
1. It is nursing staff’s responsibility to keep care-dependent clients’ natural teeth clean.
2. I feel more uncomfortable helping clients cleaning their teeth, mouth or dentures than I do with most other kinds of personal care.
3. I believe I can help in preventing my clients’ teeth from becoming decayed and getting gum disease.
4. I think that only the dentist can prevent clients’ teeth from decaying and getting gum disease.
5. Brushing teeth is a very personal thing that you should not be expected to do for somebody else.
6. In my opinion, clients need to see the dentist whether they have a problem or not.
7. When I clean my client’s teeth, mouth or dentures, I’m unsure if I am doing it right.
8. Nurses can assess clients’ oral hygiene status.
9. Nurses can assess the presence of dental caries in clients.
10. Nurses can assess the presence of periodontal disease in clients.
11. Nurses can assess clients’ level of oral health self-care.
12. Nurses should do oral health assessments to plan appropriate oral health care for clients.
13. Nurses should encourage their clients who have dental problems to see a dentist.
OHAT statements
1. The Oral Health Assessment Tool can act as a reminder to assess oral health when doing my nursing home rounds.
2. The Oral Health Assessment Tool is a quick and easy tool to use during nursing home rounds.
3. I would use the Oral Health Assessment Tool during my rounds in the nursing home.
4. The Oral Health Assessment Tool can help me recall categories of the mouth that need to be assessed therefore improving my assessment skills.
5. I could prescribe the Oral Health Assessment Tool to be used as an assessment tool in the nursing home.
Daily doses – uncut news
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


