
About the authors:Joanne Greenwood, RN, RM, is a dermatology Patricia McClunie-Trust, RN, PhD, is a principal academic staff member in the Centre for Health and Social Practice/Te Tari Hauora me Te Tari Tikanga-ā-Hapori, Waikato Institute of Technology, Hamilton. |
ABSTRACTBackground: This review explores the lived experience of people through the lens of their journey with psoriasis. Most of the efforts to understand the impact of psoriasis on a person’s life have been quantitative studies focusing on quality of life. There is a need to understand more about what it is like living with psoriasis. This understanding may provide insight into the wellbeing and health priorities of those living with psoriasis and help health professionals provide them with more holistic care. Objective: To explore the lived experiences of adults with psoriasis. Methods: A qualitative meta-synthesis was undertaken using meta-ethnography. Databases searched included CINAHL, PubMed, MedNar, Gale and Sociology Source. Qualitative studies published in English and reporting primary data analysis including the experiences of people with psoriasis were considered for inclusion. Findings: Nineteen studies were included. Three themes emerged from the synthesis about the lived experience of psoriasis, including the impact on participants’ self-identity, wellbeing and culture. Participant voices underline the daily struggles they experience, including how psoriasis is all-consuming, shaping their being, and how people with psoriasis use isolation as a coping mechanism, making themselves and their bodies invisible. Conclusion: Psoriasis affects all aspects of a person’s life. The level of understanding a health professional has of what it is like to live with psoriasis underpins and informs their therapeutic approaches and can play a pivotal role in helping a person with psoriasis successfully manage their condition. |
||
KEYWORDSpsoriasis, lived experience, self-identity, isolation, culture, wellbeing |
|||
 Joanne Greenwood
Joanne Greenwood Patricia McClunie-Trust
Patricia McClunie-TrustINTRODUCTION
THE AIM OF this review was to explore the lived experiences of people with psoriasis. Psoriasis is a common chronic debilitating long-term condition that affects millions of adults worldwide. It is estimated that approximately 90,000 people in New Zealand have been diagnosed with this condition (Health Navigator, 2023). Due to the skin being the largest and most visible organ of the human body, having blemished skin affects all aspects of a person’s quality of life and has further implications as it predisposes them to many other comorbidities. For these reasons, individuals with psoriasis experience unique psychosocial effects and encounter day-to-day challenges. Exploring the lived experiences of adults with psoriasis is an evolving area of research that has the potential to inform current clinical practice and direct population health initiatives.
BACKGROUND
World Health Organization (WHO) (2016) data suggests that the prevalence of psoriasis in all countries ranges from 0.09 per cent to 11.43 per cent of the population. Studies show that psoriasis is prevalent in adults, affecting approximately 2 per cent to 4 per cent of both males and females equally (Alzeer et al, 2022; Demir & Aksoy, 2019; Nicolescu et al, 2021). Recent literature has shown that psoriasis is a cutaneous disease linked to comorbidities like inflammatory bowel disease, cardiovascular disease, mental health disorders, diabetes mellitus, metabolic syndrome, psoriatic arthritis, hypertension and hyperlipidaemia (Daniel, 2020). Being a chronic, incurable condition, psoriasis can stretch from childhood through to old age, leading to missed opportunities in education, work, and personal life (WHO, 2016). Psoriasis burdens individuals with stigma and discrimination, undermining self-confidence and self-image.
Treatment for psoriasis is based on the severity, body surface area it covers and the clinician. Kalb (2019) suggests that with a limited surface area of <3 per cent, treatment should be topical therapy. Another option available for treatment is phototherapy, which involves using “narrowband” ultraviolet (UVB) light (Oakley, 2001). For larger affected areas, covering more than 10 per cent of the body, systematic therapy using medications such as methotrexate, ciclosporin, acitretin or apremilast (not subsidised in New Zealand) may be indicated. Biologic systematic therapy is the subsequent line of treatment, but its usage in clinical practice is limited due to its high cost (Vather, 2020). Complementary or alternative medicines (CAM) are also commonly used by people with psoriasis, including herbal therapies, dietary supplements, mind/body interventions, climatotherapy (bathing in the Dead Sea and sunbathing for several weeks) and traditional Chinese medicines (Talbott & Duffy, 2015).
People with psoriasis tend to score lower in studies on subjective health status and psychological well-being (Reimus et al, 2007). Subjective wellbeing is defined as how people feel about their lives and their overall satisfaction with life (Cummins et al, 2009). A high level of disease severity is strongly associated with lower subjective wellbeing and depression, while improvement in skin condition was found to improve wellbeing (Schuster et al, 2022). Therefore, it is essential to evaluate the mental burden of this disease to weigh the impact of psoriasis on people’s lives (Dogan et el, 2022) and include measures of wellbeing in therapeutic approaches (Schuster et al, 2022).
Given the prevalence and long-term nature of psoriasis, along with its complex management, the objective of this meta-synthesis was to report on the lived experiences of people with psoriasis. This review will enable us to make recommendations to inform decision-making in current health practices and policies. The review question was: “What are the lived experiences of adults with psoriasis?”
METHODS
Study design
The methodological process followed in this review was informed by the meta-ethnography phases outlined by Noblit and Hare (1988). There are seven phases to completing a meta-ethnography, as shown in Table 1 (below) (France et al, 2019, p. 2).
Table 1: Meta-ethnography — seven phases
| Phase 1 | Identifying a phenomenon of interest that qualitative research might inform |
| Phase 2 | A systematic review of the literature |
| Phase 3 | Reading the studies |
| Phase 4 | Determining how the studies are related |
| Phase 5 | Translating the studies into one another |
| Phase 6 | Synthesising translations |
| Phase 7 | Expressing the synthesis |
Phase 1 – Identifying a phenomenon: A phenomenon of interest was identified, and a review question was developed. Elements of the PICo (population, phenomenon of interest, context) were identified as adults, lived experiences and psoriasis during the systematic literature review. The population was viewed as human adults; the phenomenon of interest was lived experiences and the context mechanism cause-and-effect relationship, psoriasis. The PICo is presented in Table 2 (below).
Table 2: PICo table
| Key words | Synonym and other terms | |
|---|---|---|
| P – Population | Adults | Adults |
| I – Interest, Phenomenon of | Lived experiences | Attitudes, perceptions, views, feelings, emotions, life experiences |
| Co – Context | Psoriasis | Psoriasis |
Phase 2 – Systematic review of the literature: A systematic search was carried out using five databases in August 2022. The search used the terms derived from the PICo. The entire PubMed search string used is shown in Appendix 1 (see below References) and was adapted for CINAHL, MedNar, Gale and Sociology Source.
Study selection
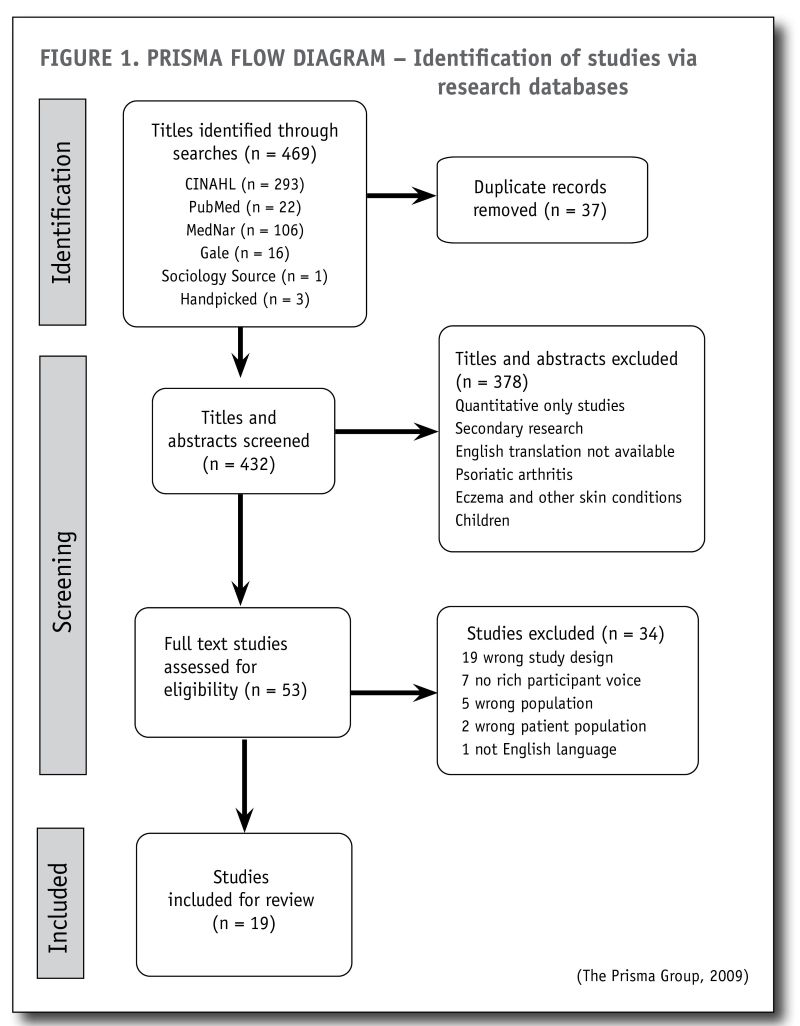
Phase 3 – Reading the studies: Inclusion and exclusion criteria were applied to the selection of studies (see Table 3, below). Primary research studies published in the last 10 years were included. Articles found to be exclusive to infants, children, adolescents or other skin conditions were excluded, along with articles not published in English unless an English translation was available. Additional relevant articles were handpicked from the reference lists of secondary research studies to add completeness and rigour. The PRISMA process diagram (Figure 1, below) shows the identification of the studies selected at each stage. Each study was critically appraised for methodological quality using the Joanna Briggs Institute (JBI, 2020) critical appraisal tool for qualitative research studies (see Appendix 2, below References).
Table 3: Inclusion/exclusion criteria
| Inclusion | Exclusion |
|---|---|
| Adults > 18 years | Children |
| Psoriasis | Eczema and other skin conditions |
| “Lived experiences” | Quantitative |
| Qualitative | Non-English language |
| English language | Grey literature |
| Within 10 years (2012-2022) | |
| Peer-reviewed primary research |
Data analysis framework
The data analysis for this meta-ethnography took place in stages four, five and six.
Phase 4 – Determining how the studies are related: The reviewers examined each study in detail, colour highlighting quotes to place the quotes from each study into sub-categories; along with metaphors, concepts or themes. Then each sub-category was synthesised, and common concepts or themes were identified. This process identified whether the accounts were directly comparable (reciprocal translations), in opposition to each other (refutational), or related studies but dissimilar, which, when taken together, represented a narrative storyline.
Phase 5 – Translating the studies into one another: The translating process entailed appraising the key concepts amid and across the studies. The reviewers examined the key concepts amid and across each study, and each concept was, in turn, juxtaposed to all the other studies to determine similarities or variances. Similarities and variances of key concepts between studies were identified, and the concepts were arranged into categories, encompassing the themes across the studies (third-order constructs) (Connery et al, 2020).
Phase 6 – Synthesising translations: The synthesis was achieved by preserving each study’s central metaphors and concepts and comparing them with the key metaphors and concepts from other studies. The synthesising of the translations produced overarching metaphors and themes from the concepts of the original studies.
Characteristics of selected studies
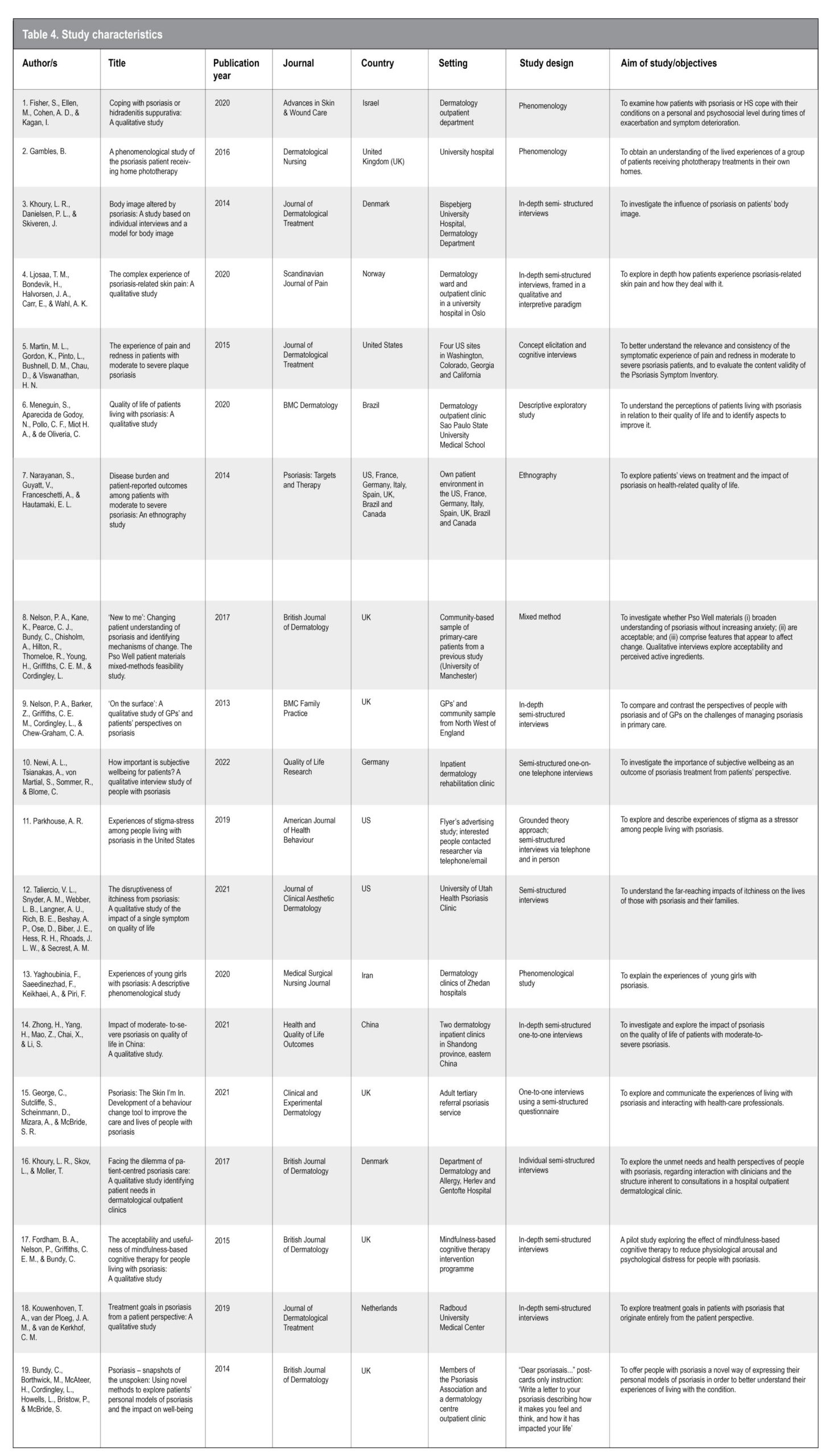
The characteristics of the 19 studies selected for inclusion in the meta-synthesis are set out in Table 4 (below). The 19 studies were published between 2013 and 2022. All studies were in English and were from differing qualitative designs consisting of: three phenomenology, two exploratory descriptive, two grounded theory, one ethnography, one mixed method, and 10 interpretive qualitative. The settings of the studies ranged from hospital inpatient and outpatient clinics, health clinics, and their own patient or home environment. Studies were done in China, Israel, Denmark, the United States, the United Kingdom, Norway, Brazil, Germany, Iran, France, Italy, Spain and Canada. No New Zealand- or Australian-based studies were found.
Phase 7 – Expressing the synthesis
FINDINGS
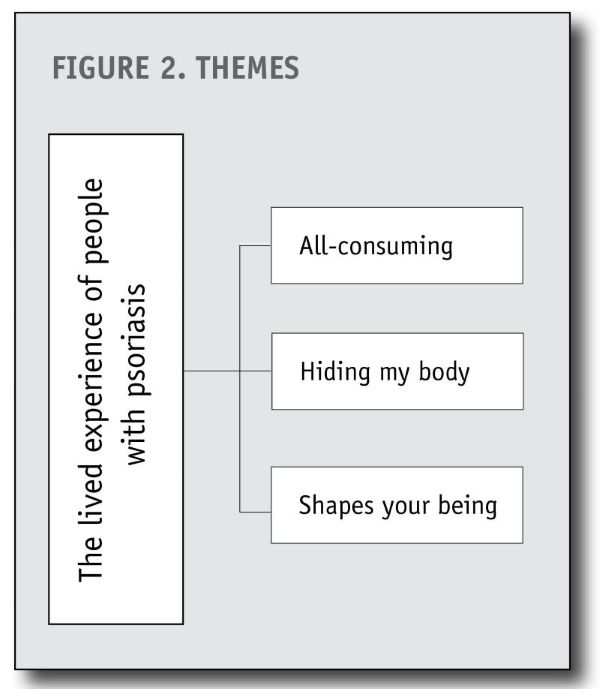
Three primary themes emerged from the synthesis, including psoriasis is all-consuming, hiding my body and psoriasis shapes your being (see Figure 2, below).
Theme 1 – All-consuming
Narrative storyline – psoriasis is uncomfortable
Psoriasis is all-consuming because it affects every aspect of a person’s life. Participants in the studies relate stories of the experience of itching, pain and the shedding of scales, all of which are constant (Fisher et al, 2020; Gambles, 2016). This intense itch can be painful and distracting, coupled with the overproduction of flaky scales that leave a trail wherever one goes, resulting in stress and anxiety for those with psoriasis (Khoury et al, 2014; Ljosaa et al, 2020).
“There’s never a moment my scalp doesn’t itch”
(Taliercio et al, 2021, participant FG P5 294, p. 47).
The sensation of constantly being itchy affects their concentration and disrupts their ability to work effectively. Participants’ stories articulate the ever-present sensation of being itchy, which makes it difficult to focus on anything else except to scratch that itch until relief is obtained (Fisher et al, 2020). The bleeding caused by scratching distracts the person, undermining their ability to concentrate effectively at work (Taliercio et al, 2021; Zhong et al, 2021).
“When I am scratching myself all day, I can’t concentrate on something else. It keeps my mind busy most of the day” (Fisher et al, 2020, participant M8pso, p. 663)
“It affects work efficiency. Let’s say if I’m working on something and touched my hair accidentally. Dandruff would fall a lot and I would feel dirty and itchy and couldn’t resist scratching. If it bleeds, my concentration on work would be directly lowered”
(Zhong et al, 2021, participant Male 2, p. 7)
Participants’ stories depict a vicious cycle of intense itching, the sort of itching that cannot be controlled, and that drives them to distraction (Fisher et al, 2020; George et al, 2021). It leaves a trail of destruction in its wake, including blood, skin, and feelings of despair and frustration. As one participant’s partner noted:
“When he needs to scratch, he will start bleeding, and he will say, ‘Oh, that’s better.’ And, within minutes, he is trying to scratch it even more while he is bleeding, and it itches so bad”
(Taliercio et al, 2021, participant FG4 FM1214-215, p. 45)
“S**t gets everywhere, like armchairs. It’s worse than a dog shedding. [My wife] asks me why I itch it, but it’s because it f***ing itches … Why can’t you just understand? I’m sorry I’m making a mess. She asks, ‘Why don’t you go to the doctor?’ I have! Nothing works”
(Taliercio et al., 2021, participant FG3 P5 225-228, p. 46)
The following studies observe feelings of revulsion and embarrassment about the trail of skin that people with psoriasis leave in their wake (George et al, 2021; Packhouse, 2019; Zhong et al, 2021).
“Everyone kept saying, ‘Oh my God will you stop itching, it’s terrible, there’s bits of your psoriasis all over the house’ ” (George, et al, 2021, participant 16, p. 4).
“[It is] extremely itchy and always has flakes falling off. In the worst time, the fallen flakes from my legs would add up to 50g. A dreadful scene”
(Zhong et al., 2021, participant Male 13, p. 4)
People with psoriasis realise that their skin shedding affects not only them but also their loved ones. Participants’ stories relate their extreme awareness of their skin flaking off, and the dreadful mess they leave in their wake, including the extra cleaning involved (Fisher et al, 2020; Packhouse, 2019).
“When I rise from a chair, I quickly check if there are scales on it and whip them away quickly. It makes me so ashamed” (Fisher et al, 2020, participant M8pso, p. 664).
“My poor wife she has a lot to put up with, all the extra cleaning and things. The bed gets covered in blood and mess; I drop scale everywhere”
(Gambles, 2016, participant Peter, p. 45).
Participants identified heat and sweat as contributing to an increased itch (Khoury et al, 2014; Taliercio et al, 2021). They have found that wearing inappropriate clothing for the weather conditions, to hide their psoriasis, leads to discomfort and increased itch.
“I have to wrap myself up in a lot of clothes, which is uncomfortable. The psoriasis flares up and starts itching” (Khoury et al., 2014, participant M4, p. 4)
“It is more itchy throughout the day if I start sweating […] or like if you are going out to exercise or something, it is more itchy to me”
(Taliercio et al., 2021, participant IT4 40-42, p. 45).
People with psoriasis tell of sleepless nights, up itching all night, unable to curtail the uncontrollable desire to scratch, and the impact of little sleep on their functioning (Fisher et al, 2020; Taliercio et al, 2021; Zhong et al, 2021).
“Even if I’m sleepy at night, I can’t fall asleep because it’s too itchy. Sometimes I wake up in the middle of the night. It’s so uncomfortable and I don’t know how to make it better”
(Zhong et al, 2021, participant Male 10, p. 4)
“It seems like I can’t remember the last time I slept eight hours in a row. So, it definitely […] affects my sleep” (Taliercio et al., 2021, participant FG2 P3 243-245, p. 46)
“The itch from my psoriasis prevents me from sleeping. It makes me be agitated most of the time”
(Fisher et al, 2020, participant F3pso, p. 664).
Some participants feel that psoriasis-associated pain is easier to deal with than itch, as pain can be controlled, whereas they have found no way to stop the incessant itch (Martin et al, 2015; Taliercio et al, 2021). Others find that pain distracts them from the itch; however, psoriasis-related pain also prevents them from doing things they did in the past (Taliercio et al, 2021; Zhong et al, 2021).
“But I would much rather hurt than itch, and so I do scratch until it hurts and then it doesn’t itch anymore. […] it’s easier to deal with the pain”
(Taliercio et al., 2021, participant FG1 P1 508-509, p. 47)
“There [are] a lot of things we used to do [that now] we just can’t because she is having pain and itching and she is not comfortable going out with all of the sores and plaques all over her body and bleeding all over everything”
(Taliercio et al., 2021, participant FG4 FM2 36-39 41-44, p. 46)
Theme 2 – Hiding my body
Narrative storyline – The notion of visibility
People living with psoriasis struggle with the visibility of their bodies in the world. The theme “hiding my body” characterises ideas about making the body invisible, encompassing the feelings and fears about being visible.
“Living with psoriasis is horrible because it is so visible” (Kouwenhoven et al, 2019, participant F5, p. 16)
“You can’t hide psoriasis; it is like a sign on your face and hands” (Fisher et al, 2020, participant M10pso, p. 665)
People with psoriasis hide their bodies because being visible attracts unwanted attention and rejection, making them feel ugly, ashamed, stigmatised and like a leper.
“I don’t want to display myself. I have seen how other people with psoriasis appear. They are white and disgusting.”
(Khoury et al, 2014, participant W2, p. 4)
They tell stories about hiding their bodies in various ways: covering up with clothing, controlling how much they expose their body, or withdrawing from social interactions and activities and isolating themselves (Fisher et al, 2020; Gambles, 2016). Even the simple natural movement of an arm is restricted (Gambles, 2016; Khoury et al, 2014).
“I have rashes on the underside of my arm, so I try not to raise my arm…”
(Khoury et al, 2014, participant W3, p. 4)
“I have been hiding myself for a year, from anyone and from the outside world. I didn’t invite people over either because I thought I would have to clean up all the flakes. So nobody visited me. My home didn’t feel like home, it was just the place where I slept, like a den.”
(Kouwenhoven et al, 2019, participant M3, p. 16)
People with psoriasis expressed anxiety at being seen as a person covered in a red, scaly, flaky unpleasant rash:
“You’re desperate for people not to notice. So, I took my socks off, and all the kids went ‘Aaah’ … too late by then. I had been seen.”
(Gambles, 2016, participant Rose, p. 45)
People with psoriasis feel unable to wear the clothes they want, as they feel that people are looking at them.
“You can’t wear what you want; you become embarrassed about going swimming or to the gym, and you feel that people are looking at you.”
(Gambles, 2016, participant Lisa, p. 45)
Participants reported that other people stare and comment about their unpleasant appearance of psoriasis, intimating that they are afraid they may catch something, so they distance themselves from the person with psoriasis (George et al, 2021; Yaghoubinia et al, 2019; Zhong et al, 2021). Participants said that because of the misconceptions associated with this skin condition, people are revolted and afraid (Newi et al, 2022; Parkhouse, 2019). A participant told of the experience at a gas station paying for the petrol, handing over the money.
“She saw my hand, which was covered full-blown in psoriasis scales, and she looked at my hand, looked at me, and put my change on the counter.”
(Parkhouse, 2019, participant Beth, p. 250)
Other people’s adverse reactions reinforce the internal struggles people with psoriasis face about their self-image and worth. This leads to self-preservation actions, such as hiding their body and isolating themselves, to avoid further attacks on an already fragile body image and self-esteem (Gambles, 2016; Narayanan et al, 2015).
“You feel like you should have a bell ringing as you’re walking … like a leper.”
(Gambles, 2016, participant Jim, p. 46)
“… I would never shower in a public changing room … I won’t give people the opportunity to think: ‘Yuk, what’s that?’.”
(Khoury et al, 2014, participant W1, p. 5).
For some, looking at themselves in the mirror is a daily struggle, even if it is sometimes necessary to ensure they are not bleeding or the psoriasis patches are not exposed (Khoury et al, 2017; Narayanan et al, 2015). They hide their bodies as they feel ugly, ashamed and unattractive.
“I am too embarrassed to be naked, even in the dark.” (Fisher et al, 2020, participant M11pso, p. 664)
“I don’t want to look at my body … My eyes focus on my face, and I control my eyes, so they don’t slide down.” (Khoury et al, 2014, participant W1, p. 6)
Participants say they crave feeling and being normal, not being abnormal and different (Fisher et al, 2020; Meneguin et al, 2020). They say that looking “normal” means healthy and that the presence of psoriasis somehow makes them unhealthy. A participant said that after taking a shower,
“For a short time, my skin looks normal, without the ugly scales, and for a few minutes, I look healthy. I really like this feeling.”
(Fisher et al, 2020, participant F7pso, p. 665)
They express feelings of sorrow and of wanting to vanish – vanish so that they are alone and do not need to pretend that they are alright. Alone, they do not need to feel shame as no one can see them; they can cry and feel sorry for themselves (Fisher et al, 2020; Parkhouse, 2019).
“You constantly feel like a part of you is broken or different, nobody wants to feel different.”
(Parkhouse, 2019, participant Alan, p. 248)
Participants paint a picture of psoriasis being a “very hidden condition” (Parkhouse, 2019), hidden by the participants themselves and not publicised in the media to promote public understanding. Participants wish for an understanding they liken to how the media has facilitated a worldwide understanding of cancer.
“Quality of life could be improved by making other people aware that a person with psoriasis on their skin does not have a disease transmitted by sight, by clothing, by soap, in any way … Because people stare and are disgusted and scared, but that is a problem that person has. I think that is the reason why a lot of people suffer … to see the prejudice of others.”
(Meneguin et al, 2020, participant DCS, p. 3)
Theme 3 – Shapes your being
Narrative storyline – Psoriasis has an emotional impact
These stories tell how a person’s being is shaped by the emotional impact of psoriasis. Withdrawal from social circles commonly occurs, exacerbated by the reactions and reception of others and the inward struggles with changes to body image (Fisher et al, 2020; Gambles, 2016).
“It really connects to your being, and then how you evolve as a human being is with the psoriasis dictating it. It shapes you.”
(Gambles, 2016, participant Rose, p. 45)
Participants describe how psoriasis shapes their social interactions with other people in ways that have implications for the whole breadth and scope of life (Khoury et al, 2017; Meneguin et al, 2020). They are embarrassed by the appearance of their skin condition and are subjected to stigmatism because of it. The anxiety they feel when socialising, defines and shapes them as a person. Participants express a profound sense of self – this is who I am now, because I have psoriasis.
“I don’t go to friends’ gatherings anymore. Sometimes it shows even on my face and I feel embarrassed to go out. If I go have lunch with my friends, and the skin flakes keep falling off, I couldn’t be at ease. Even if there were no flakes, there would be white patches on the skin. I fear it would disgust others.”
(Zhong et al, 2021, participant Female 17, p. 6).
Socialisation through employment can provide a sense of accomplishment, identity, and connection with people. Participants expressed a sense of loss of their former self and their identity within the community and workplace, and felt a reluctant acceptance that life would never be the same, that they would never be the same (Fisher et al, 2020; Narayanan et al, 2015).
“That’s how I used to look [points at picture on mantelpiece], it’s like I miss myself. Running things, being in charge, being in the office, being up in management and now I’m just like this now.”
(Narayanan et al, 2015, participant Female US, p. 3).
“Can I go to a job interview with face full of scales? Can I represent myself as a dignified academic person without shaking hands? Wearing a long sleeve shirt in summertime?”
(Fisher et al, 2020, participant M10pso, p. 666).
Their appearance had changed and with it their sense of self.
“I wish my body was as before, without psoriasis. My body was clean and perfect … I used to be a handsome guy, and then all of a sudden, I became a completely different person. I hate my psoriasis.”
(Khoury et al, 2014, participant M1, p. 5)
Psoriasis affects the relationships people with psoriasis have with others. Participants in the studies reflected on the difficulties of: putting themselves out there with a prospective partner; telling their prospective partner that they have psoriasis; showing them their body; involving them in “life” with psoriasis; or just maintaining an existing relationship that started before developing psoriasis (Yaghoubinia et al, 2020; Zhong et al, 2021). They also talked about internal struggles with body image and self-loathing. As participants noted:
“… people’s reactions, girls’ reactions … it’s your self-consciousness of it. That could be quite overwhelming at points.”
(Nelson et al, 2013, participant P1, p. 5)
“I don’t sleep on the same bed with my wife. I sleep in another room. I have my own bed with sheets and blankets of my own. I isolate myself from my family. There’s no other way. I loathe myself.”
(Zhong et al, 2021, participant Male 22, p. 6)
Participants reported their partners’ responses to the manifestation of psoriasis.
“I have a kind husband, who tells me I look pretty, but it’s difficult to believe … I definitely prefer the light to be switched off, and if not, I avoid looking at myself.”
(Khoury et al, 2014, participant W3, p. 4)
Participants highlighted the emotional remodelling and reshaping that takes place through the reactions of others to their skin condition. Those reactions help shape how they perceive that society views them and also in how they view themselves, changing and reshaping their being (George et al, 2021; Khoury et al, 2017).
“They get uncomfortable and afraid that it might be contagious. A girl in a fitness centre shouted out loud that I was disgusting.”
(Khoury et al, 2014, participant W1, p. 5)
“It is quite isolating, it’s hard to just deal with the skin disease and then also dealing with your emotions … it’s a bit like a split personality.”
(George et al, 2021, participant 10, p. 5)
Participants also said that psoriasis alters their appearance, and in learning to cope with their “new” appearance, their being is reshaped.
“I once had a session with a psychologist, because I needed help to accept my body.”
(Khoury et al, 2014, participant W3, p. 5)
Participants have pointed out that help is needed. Education about psoriasis and the psychological aspects that impact a person with the condition may be vital in removing some of the stigma around body image, helping to remove the social isolation they experience daily.
“They need to teach people that have this illness, what this illness does to you, and what to look out for so that you can mentally cope with this illness.”
(George et al, 2021, participant 7, p. 6)
“Physically, today, I can say that I am rid of it. But psychologically I think I am not rid of it. If I really started thinking about all of this, I think I’d fall into depression. I can’t say that today my psoriasis is in the past – even if it’s no longer visible.”
(Narayanan et al, 2015, participant Female France, p. 3).
DISCUSSION
This meta-synthesis sought to explore the lived experiences of adults with psoriasis. We identified 19 studies exploring the impact of psoriasis on participants’ lives. The findings of this synthesis reveal how psoriasis impacts every aspect of a person’s life and wellbeing. There is no universally accepted definition of wellbeing, due to different cultures valuing different concepts and perspectives (Mayberry et al, 2022). However, the World Health Organization (2020) defines wellbeing as “a state of complete physical, mental and social wellbeing, and not merely the absence of disease or infirmity” (para. 5). How we know ourselves is through our human interconnectedness and our position within society.
Wellbeing can be linked to a sense of purpose and belonging. Everyone wants to belong, in society, as part of a family, in social circles, and within a work environment. However, having psoriasis can lead to being socially displaced, excluded or marginalised and can cause existential health-related ruptures in people’s lives. Psoriasis influences people’s physical health as well as their psychological and psychosocial wellbeing. People with psoriasis often feel like lepers, displaced from where they belong and they struggle for re/emplacement and re/integration into their places of belonging (Mattes & Lang, 2021).
Douglas (1966) refers to this social displacement as creating a marginal state for people with psoriasis, who are perceived as dangerous. Social displacement results in a loss of belonging, and self-stigmatisation. This social displacement comes from the perception that people with psoriasis are dangerous, in terms of being infectious, contagious or unclean. Self-stigmatisation is the outcome of negative self-talk. It can lead to feelings of unworthiness, to the person self-isolating for fear of rejection and to an altered body image, all of which are associated with depression (Weinberger et al, 2021). People with psoriasis experience a transition in identity from their old self without psoriasis to the new self with psoriasis. This transition positions them outside their previous place of belonging and security, and into a marginal state, with society declaring their new status as unacceptable and to be feared.
Wellbeing can be affected through diminished identity and self-esteem. This diminished identity often leads to negative emotions like shame and self-loathing that lead to withdrawal from leisure and social activities, which then further diminishes self-esteem, creating a vicious cycle (Synard & Gazzola, 2018). It can be argued that the interconnected characteristics of identity, including culture, community, work, and belonging, are fundamental to wellbeing and that any disruption to any of these characteristics can be detrimental (Gall et al, 2021). Therefore, the balance of one’s mental, physical, emotional and spiritual aspects of life is essential to one’s wellbeing.
Psoriatic skin lesions can appear threatening because they can be interpreted as being contagious or infectious and therefore unsafe in proximity (Almeida et al, 2017). Consequently, people with psoriasis find themselves in what anthropologists call a liminal space. Liminality is derived from an inability to classify people as one thing or the other, or to position them in the cultural or social space in which they are normally located (Douglas, 1966). Multiple factors contribute to liminality, including the struggle about where self-identity and psoriasis overlap. The removal of a person from their identified cultural space has implications for their wellbeing (Gall et al, 2021).
Wellbeing measures are often underpinned by Western philosophical concepts and do not consider indigenous concepts of wellbeing (Gall et al, 2021). People with psoriasis have their own concepts of health and wellbeing, drawn from their own experiences and shaped by socialisation and social interactions. Their values and beliefs are shaped by the environment and worldwide views about image, and about being clean and touchable. Being healthy means being seen as “normal”, with normal skin, even if this is an illusion brought about by a shower or through longer-lasting treatment options.
People with psoriasis rapidly become aware of others’ aversion to the sight of their skin rash, and they attempt to hide it. They hide to normalise themselves, so they do not stand out as a “person out of place” in their interactions with others (Douglas, 1966). As a cultural and social concept, stigma is associated with the skin’s appearance. The visible rash on the skin acts as a mark of something seen by others as repulsive, and creates feelings of disgust. This is a form of deep-seated social control constantly reinforced by social media (Magin et al, 2010). Social media portrays images of beautiful clear skin as the socially accepted norm, an image that those with psoriasis fail to meet. Social exposure, and consequent rejection based on skin appearance, create apprehension, anxiety and fear of intimacy in people with psoriasis (Lahousen et al, 2016). Having visible skin lesions causes psychological trauma, as the person realises they are no longer socially acceptable and feel out of place, leading to the self-isolating behaviour exhibited by those with psoriasis (Kowalewska et al, 2019).
Douglas (1966) describes the idea of “matter out of place”, which is thought-provoking when applied to the shedding of skin experienced by those with psoriasis. Matter out of place is often perceived to be unclean in a cultural sense. Socially and culturally, skin shedding produces feelings of revulsion and a sense of uncleanliness, of the individual themselves, but also the environment they function in. The feelings of revulsion and uncleanliness lead to less-than-ideal situations at work and home where the person with psoriasis experiences aversion to the skin scale they leave in their wake. This aversion produces a connection between the marked body and danger, creating an anxious state of being, as they try to conceal or get rid of the evidence of uncleanliness which is socially and culturally unacceptable. The inability to control the visible symptoms of their skin condition drives people with psoriasis to remove themselves from situations where they may be stigmatised further, again generating isolating behaviour (Bundy et al, 2014).
A priority for people with psoriasis may be to try and make the appearance of the skin look more normal and reduce physical symptoms like flaking and itching. Health professionals need to understand what it is like to live with psoriasis daily. If they do, it will help them understand the priorities of people with psoriasis and the burdens they face daily. Insights into the lived experience of psoriasis could lead to improvements in the provision of care, treatment and support (Nash et al, 2015). If people with psoriasis can access therapeutic intervention (such as biologic medications) to control the visible symptoms of psoriasis, creating the appearance of normal skin, will this then enable them to move out of the liminal space, as they are no longer a “matter out of place”, a leper in society, but a “normal person”?
Education is fundamental to the wellbeing of people with psoriasis and should be seen as a therapeutic intervention to help them understand and manage their condition. However, education should not just support the physical condition (Aldeen & Basra, 2011). The findings of this synthesis highlight that people with psoriasis need education and support with the psychological and psychosocial impacts of psoriasis. They need support to enable them to shift from the liminal and “matter out of place” space. Nurses are positioned to play a pivotal role in delivering ongoing education and support for people with psoriasis. Just as psoriasis is multifaceted, so is the understanding needed to treat and promote wellbeing for people with psoriasis.
RECOMMENDATIONS
- Primary New Zealand research is needed to further explore the cultural meanings and implications of psoriasis.
- Research should also explore health professionals’ understanding of what it is like to live with psoriasis and how that understanding informs therapeutic approaches.
- Education for nurses is also essential to develop and widen their knowledge and understanding of skin conditions and the impact they have on wellbeing. This knowledge could help develop and inform current clinical practice.
- Health literacy education should be offered to people with psoriasis, to help them understand the therapeutic purpose of interventions.
- Health professionals need to be informed about what support groups are available for people with psoriasis in their region.
LIMITATIONS
This review offers interpretations of the meaning of living with psoriasis. A limitation may be that only qualitative studies were included in this synthesis. There may be findings from quantitative studies that provide different perspectives about living with psoriasis, including quality of life and wellbeing measures. While psoriasis is more dominant in people of European descent, it is present in all ethnicities. The cultural meanings and implications of psoriasis were not identified in the studies included in this synthesis.
CONCLUSION
This meta-ethnography identified and synthesised primary qualitative research literature on people’s experiences with psoriasis. The findings from 19 studies spanning 10 years were synthesised and developed into storylines. In these stories, participants described a complex picture with a rich narrative of being all-consumed by psoriasis, wanting to hide their body and the fact that psoriasis shaped their being. These powerful narratives reveal important insights into how people live with psoriasis as a long-term condition.
ACKNOWLEDGEMENTS
The authors acknowledge Mellisa Chin for her assistance in developing the manuscript for publication.
REFERENCES
Aldeen, T., & Basra, M. (2011). Management of psoriasis and its comorbidities in primary care. British Journal of Nursing, 20(18), 1186-1192.
Almeida, V., Taveira, S., Teixeira, M., Almeida, I., Rocha, J., & Teixeira, A. (2017). Emotion regulation in patients with psoriasis: Correlates of disability, clinical dimensions, and psychopathology symptoms. International Journal of Behavioural Medicine, 24, 563-570.
Alzeer, F., AlOtair, H., & Aleisa, A. (2022). Epidemiology and cutaneous manifestations of psoriasis in Saudi Arabia: A narrative review. Clinical, Cosmetic and Investigational Dermatology, 15, 347-355.
Bundy, C., Borthwick, M., McAteer, H., Cordingly, L., Howells, L., Bristow, P., & McBride, S. (2014). Psoriasis – snapshots of the unspoken: Using novel methods to explore patients’ personal models of psoriasis and the impact on well-being. British Journal of Dermatology, 171(4), 825-831.
Connery, A., McCurtin, A., & Robinson, K. (2020). The lived experience of stuttering: A synthesis of qualitative studies with implications for rehabilitation. Disability and Rehabilitation, 42(16), 2232-2242.
Cummins, R. A., Mellor, D., Stokes, M., & Lau, A. L. (2009). Measures of subjective well-being. In E. Mpofu & T. Oakland (Eds.), Rehabilitation and health assessment: Applying ICF guidelines (pp. 409-426). Springer Publishing Company.
Daniel, B. (2020). The multiple comorbidities of psoriasis: The importance of a holistic approach. Australian Journal of General Practice, 49(7), 433–437.
Demir, M., & Aksoy, M. (2019). The retrospective evaluation of clinical and demographic features of children with psoriasis. Journal of Harran University Medical Faculty, 16(2), 321-325.
Dogan, Y., Killic, F. A., & Ozcelik, S. (2022). Anxiety, Depression, and Sexual Dysfunction in Patients with Psoriasis. Turkish Society of Dermatology, 16, 62-69.
Douglas, M. (1966). Purity and danger: An analysis of concepts of pollution and taboo. Routledge.
Fisher, S., Ellen, M., Cohen, A. D., & Kagan, I. (2020). Coping with psoriasis or hidradenitis suppurativa: A qualitative study. Advances in Skin and Wound Care, 33, 662-668.
France, E. F., Cunningham, M., Ring, N., Uny, I., Duncan, E. A. S., Jepson, R. G., Maxwell, M., Roberts, R. J., Turley, R. L., Booth, A., Britten, N., Flemming, K., Gallagher, I., Garside, R., Hannes, K., Lewin, S., Noblit, G. W., Pope, C., Thomas, J., Vanstone, M., Higginbottom, G. M. A., & Noyes, J. (2019). Improving reporting of meta-ethnography: The eMERGe reporting guidance. Psycho-Oncology, 28, 447–458.
Fordham, B. A., Nelson, P., Griffiths, C. E. M., & Bundy, C. (2015). The accessibility and usefulness of mindfulness-based cognitive therapy for people living with psoriasis: A qualitative study. British Journal of Dermatology, 172, 805-840.
Gall, A., Anderson, K., Howard, K., Diaz, A., King, A., Willing, E., Connolly, M., Lindsay, D., & Garvey, G. (2021). Wellbeing of Indigenous peoples in Canada, Aotearoa (New Zealand) and the United States: A systematic review. International Journal of Environmental Research and Public Health, 18(5832), 1-31.
Gambles, B. (2016). A phenomenological study of the psoriasis patient receiving home phototherapy. Dermatological Nursing, 15(2), 42-47.
George, C., Sutcliffe, S., Scheinmann, D., Mizara, A., & McBride, S. R. (2021). Psoriasis: The skin I’m in. Development of a behaviour change tool to improve the care and lives of people with psoriasis. Clinical and Experimental Dermatology, 46(5), 1-8.
Health Navigator. (2023). Psoriasis – Mate tongatonga uri.
Joanna Briggs Institute. (2020). Checklist for qualitative research: Critical appraisal tools for use in JBI systematic reviews. JBI Global.
Kalb, R. E. (2019). Overcoming challenges in the management of psoriasis: Treatment advances to improve standard of care. Journal of Managed Care Medicine, 22(4), 63-66.
Khoury, L. R., Danielsen, P. L., & Skiveren, J. (2014). Body image altered by psoriasis. A study based on individual interviews and a model for body image. Journal of Dermatology Treatment, 25, 2-7.
Khoury, L. R., Skov, L., & Moller, T. (2017). Facing the dilemma of patient-centred psoriasis care: A qualitative study identifying patient needs in dermatological outpatient clinics. British Journal of Dermatology, 177(2), 436-444.
Kouwenhoven, T. A., van der Ploeg, J. A. M., & van de Kerkhof, C. M. (2019). Treatment goals in psoriasis from a patient perspective: A qualitative study. Journal of Dermatological Treatment, 31(1), 13-17.
Kowalewska, B., Gawek, N., & Kowalewska, J. (2019). Quality of life and stigmatisation of people with psoriasis. Progress in Health Sciences, 9(1), 132-136.
Lahousen, T., Kupfer, J., Gieler, U., Hofer, A., Linder, M. D., & Schut, C. (2016). Differences between psoriasis patients and skin-healthy controls concerning appraisal of touching, shame and disgust. Acta Dermato-Venereologica, 217, 78-82.
Ljosaa, T. M., Bondevik, H., Halvorsen, J. A., Carr, E., & Wahl, A. K. (2020). The complex experience of psoriasis-related skin pain: A qualitative study. Scandinavian Journal of Pain, 20(3), 491-498.
Magin, P., Heading, G., Adams, J., & Pond, D. (2010). Sex and the skin: A qualitative study of patients with acne, psoriasis and atopic eczema. Psychology, Health & Medicine, 15(4), 454-462.
Martin, M. L., Gordon, K., Pinto, L., Bushnell, D. M., Chau, D., & Viswanathan, H. N. (2015). The experience of pain and redness in patients with moderate to severe plaque psoriasis. Journal of Dermatological Treatment, 26(5), 401-405.
Mattes, D., & Lang, C. (2021). Embodied belonging: In/exclusion, health care, and well-being in a world in motion. Culture, Medicine and Psychiatry, 45(1), 2-21.
Mayberry, K., Zapata, L. V., Byers, M., & Thurston, M. M. (2022). A scoping review of well-being assessment and interventions in student pharmacists. American Journal of Pharmaceutical Education, 86(6), 743-758.
Meneguin, S., de Godoy, N. A., Pollo, C. F., Miot, H. A., & de Oliveira, C. (2020). Quality of life of patients living with psoriasis: A qualitative study. BMC Dermatology, 20(22), 1-6.
Narayanan, S., Guyatt, V., Franceschetti, A., & Hautamaki, E. L. (2014). Disease burden and patient reported outcomes among patients with moderate to severe psoriasis: An ethnography study. Psoriasis: Targets and Therapy, 5, 1-7.
Nash, A. S., McAter, H., Schofield, J., Penzer, R., & Gilbert, A. K. (2015). Psoriasis today: Experiences of the healthcare and impact on quality of life in a major UK cohort. Primary Health Care Research & Development, 16, 415-423.
Nelson, P. A., Barker, Z., Griffiths, C. E. M., Cordingley, L., & Chew-Graham, C. A. (2013). ‘On the surface’: A qualitative study of GPs’ and patients’ perspectives on psoriasis. BMC Family Practice, 14(158), 1-10.
Nelson, P. A., Kane, K., Pearce, C. J., Bundy, C., Chrisholm, A., Hilton, R., Thorneloe, R., Young, H., Griffiths, C. E. M., & Cordingley, L. (2017). ‘New to me’: Changing patient understanding of psoriasis and identifying mechanisms of change. The Pso Well patient materials mixed-methods feasibility study. British Journal of Dermatology, 177, 616-617.
Newi, A. L., Tsianakas, A., von Martial, S., Sommer, R., & Blome, C. (2022). How important is subjective well-being for patients? A qualitative interview study of people with psoriasis. Quality of Life Research, 1-9.
Nicolescu, A. C., Bucur, S., Giurcaneanu, C., Gheuca-Solovastru, L., Constantin, T., Furtunescu, F., Ancuta, I., & Constantin, M. M. (2021). Prevalence and characteristics of psoriasis in Romania – First study in overall population. Journal of Personalized Medicine, 11(523), 1-12.
Noblit, G. W., & Hare, R. D. (1988). Meta-ethnography: Synthesizing qualitative studies. Sage.
Oakley, A. (2001). Narrowband UVB phototherapy. [Dermnet NZ].
Parkhouse, A. R. (2019). Experiences of stigma-stress among people living with psoriasis in the United States. American Journal of Health Behaviour, 43(2), 243-257.
Reimus, J. L. M., Vingerhoets, A. J. J. M., Soons, P. H. G. M., & Korstanje, M. J. (2007). Suffering in psoriasis patients: Its relation with illness severity and subjective well-being. International Journal of Dermatology, 46(10), 1042-1045.
Schuster, B., Peifer, C., Ziehfreund, S., Tizek, L., Biedermann, T., Zink, A., & Schielein, M. C. (2022). Happiness and depression in psoriasis: A cross-sectional study in Germany. Quality of Life Research, 31(6), 1-13.
Synard, J., & Gazzola, N. (2018). Moving towards positive well-being in the face of adversity: What explains individual variations in well-being following job loss? International Journal for the Advancement of Counselling, 41, 415-435.
Talbott, W., & Duffy, N. (2015). Complementary and alternative medicine for psoriasis: What the dermatologist needs to know. American Journal of Clinical Dermatology, 16, 147-165.
Taliercio, V. L., Snyder, A. M., Webber, L. B., Langner, A. U., Rich, B. E., Beshay, A. P., Ose, D., Biber, J. E., Hess, R., Rhoads, J. L. W., & Secrest, A. M. (2021). The disruptiveness of itchiness from psoriasis: A qualitative study of the impact of a single symptom on quality of life. Journal of Clinical and Aesthetic Dermatology, 14(6), 42-48.
The PRISMA Group. (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Vather, D. (2020). Guidelines for the management of psoriasis. Dermnet NZ.
Weinberger, N. A., Mrowietz, S., Luck-Sikorski, C., von Spreckelsen, R., John, S. M., Sommer, R., Augustin, M., & Mrowietz, U. (2021). Effectiveness of a structured short intervention against stigmatisation in chronic visible skin diseases: Results of a controlled trial in future educators. Health Expectations, 24(5), 1790-1800.
World Health Organization. (2016). Global report on psoriasis.
World Health Organization. (2020, November 24). Assembly of parties of the International Development Law Organization.
Yaghoubinia, F., Saeedinezhad, F., Keikhaei, A., & Piri, F. (2020). Experiences of young girls with psoriasis: A descriptive phenomenological study. Medical-Surgical Nursing Journal, 8(4), 1-10.
Zhong, H., Yang, H., Mao, Z., Chai, X., & Li, S. (2021). Impact of moderate-to-severe psoriasis on quality of life in China: A qualitative study. Health and Quality of Life Outcomes, 19(1), 1-9.
APPENDIX 1
Box 1: PubMed search
| Search # | 17/08/22 | |
|---|---|---|
| 1 | Title/abstract | Adult |
| 2 | MeSH terms | Adult |
| 3 | S1 OR S2 | |
| 4 | Title/abstract | Experiences OR “lived experiences” OR attitudes OR perceptions OR views OR feelings OR emotions OR “life experiences” |
| 5 | MeSH terms | (“experiences” [MeSH Terms]) OR (“attitude” [MeSH Terms]) OR (“emotions” [MeSH Terms]) |
| 6 | S4 OR S5 | |
| 7 | Title/abstract | Psoriasis |
| 8 | MeSH | Psoriasis |
| 9 | S7 OR S8 | |
| 10 | S3 AND S6 AND S9 | |
| Add filters | 2012-2022 |
APPENDIX 2
Quality appraisal of studies using JBI Checklist for Qualitative Research
| Author (year) | Title | Qu 1 | Qu 2 | Qu 3 | Qu 4 |
Qu 5 |
Qu 6 |
Qu 7 | Qu 8 | Qu 9 | Qu 10 |
Dependability |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fisher et al (2020) | Coping with psoriasis or hidradenitis: suppurativa: A qualitative study | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | High |
| Gambles (2016) | A phenomenological study of the psoriasis patient receiving home phototherapy | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| Khoury et al (2013) | Body image altered by psoriasis: a study based on individual interviews and a model for body image | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | Moderate |
| Ljosaa et al (2020) | The complex experience of psoriasis-related skin pain: A qualitative study | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | Moderate |
| Martin et al (2015) | The experience of pain and redness in patients with moderate to severe plaque psoriasis | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | No | Yes | Moderate |
| Meneguin et al (2020) | Quality of life of patients living with psoriasis: A qualitative study | Yes | Yes | Yes | Yes | Yes | Yes | Yes1 | No | Yes | Unclear | Moderate |
| Narayanan et al (2015) | Disease burden and patient reported outcomes among patients with moderate to severe psoriasis: An ethnography study | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Moderate |
| Nelson et al (2017) | ‘New to me’: Changing patient understanding of psoriasis and identifying mechanisms of change. The Pso Well patients materials mixed-methods study |
Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | Moderate |
| Nelson et al (2013) | ‘On the surface’: A qualitative study of GPs’ and patients’ perspectives on psoriasis | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | Moderate |
| Newi et al (2022) | How important is subjective well-being for patients? A qualitative interview study of people with psoriasis | Yes | Yes | Yes | No | Yes | Yes | Yes | No2 | Yes | Yes | Low |
| Parkhouse (2019) | Experiences of stigma-stress among people living with psoriasis in the United States | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Moderate |
| Taliercio et al (2021) | The disruptiveness of itchiness from psoriasis: A qualitative study of the impact of a single symptom on quality of life | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | High |
| Yaghoubinia et al (2019) | Experiences of young girls with psoriasis: A descriptive phenomenological study | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | Low |
| Zhong et al (2021) | Impact of moderate to severe psoriasis on quality of life in China: a qualitative study | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | High |
| George et al (2021) | Psoriasis: The skin I’m in. Development of a behaviour change tool to improve the care and lives of people with psoriasis | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | High |
| Khoury et al (2016) | Facing the dilemma of patient-centered psoriasis care: a qualitative study identifying patient needs in dermatological outpatient clinics | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Moderate |
| Fordham et al (2014) | The acceptability and usefulness of mindfulness-based cognitive therapy for people living with psoriasis: A qualitative study | Yes | Yes | Yes | Unclear | Unclear | No | No | No | No | Yes | Low |
| Kouwenhoven et al (2020) | Treatment goals in psoriasis from a patient perspective: a qualitative study | Yes | Yes | Yes | Yes | Yes | Unclear | No | Yes | Yes | Yes | Moderate |
| Bundy et al (2014) | Psoriasis — snapshots of the unspoken: Using novel methods to explore patients’ personal models of psoriasis and the impact on well-being | Yes | Yes | Yes | Yes | Yes | Unclear | No | Yes | Yes | Yes | High |
NOTES
Quality appraisal tool questions:
- Congruity between the stated philosophical perspective and the research methodology.
- Congruity between the research methodology and the research question or objectives.
- Congruity between the research methodology and the methods used to collect data.
- Congruity between the research methodology and the representation and analysis of data.
- There is congruence between the research methodology and the interpretation of results.
- Locating the researcher culturally or theoretically.
- Influence of the researcher on the research, and vice-versa, is addressed.
- Representation of participants and their voices.
- Ethical approval by an appropriate body.
- Relationship of conclusions to analysis, or interpretation of the data.
Subscript notes:
- Individual participants are not clearly identified.
- Minimal reporting of participant voices.
Daily doses – uncut news
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


