
About the authors:Elyse Sibley, BN, PostGradCert, MP candidate, is a clinical nurse specialist in complex care, at Te Whatu Ora Hauora a Toi Bay of Plenty. Christine Mercer, RN, BA(SocSci), MEd, PhD, PostGradCert ProfPrac, is an academic staff member at Wintec/Te Pūkenga, Hamilton. This article was accepted for publication in September 2023. |
ABSTRACTBackground: Behavioural and psychological symptoms of dementia (BPSD) describes any agitation, aggression or escalated behaviours in a person with dementia. Recommended best practice for managing challenging BPSD is the use of nonpharmacological interventions in the first instance. Antipsychotic PRN medication is not recommended as a first-line intervention, and yet it is often used in this way. Aim: In this study, we used an integrative review to investigate why it may be challenging for staff to use nonpharmacological interventions for managing BPSD, leading them to rely on antipsychotics. Methods: The review process was based on Whittemore and Knafl’s (2005) steps for conducting an integrative review. Articles that studied the use of PRN anti-psychotics, or non-pharmacological interventions, were accessed and analysed. Inclusion criteria were a focus on older adults, with a diagnosis of BPSD who were prescribed PRN anti-psychotic medication as well as non-pharmacological interventions and were hospitalised in aged residential care/acute settings. Excluded from the study were references to younger patients, those with dementia but not BPSD, and those living at home. Results: Three themes emerged from the review: Low staff-to-patient ratios increased instances of problems with BPSD; numbers of staff with specialised training were low; and there was a need to educate staff further about the manifestation of BPSD and the implementation of person-centred care plans. Overall, use of care plans, focused on the individual, reduced use of PRN antipsychotics. Conclusions: The management of BPSD is complicated by a mix of low staffing, and/or inadequate training opportunities, leading to increased risk for both the individual and possible staff burnout. The research has shown an increase in education/training reduces these risks when paired with implementation of non-pharmacological care plans. |
||
KEYWORDSbehavioural and psychological symptoms of dementia, non-pharmacological interventions, behaviour management plans, aged residential care, acute psychotic older adult, nursing care |
|||


INTRODUCTION
DEMENTIA IS A TERM used to describe groups from more than 100 irreversible degenerative brain diseases with no cure. Each individual disease has its own symptoms; however, some are grouped together (Cloak & Al Khalili, 2022). The group that is the subject of this study is referred to as behavioural and psychological symptoms of dementia (BPSD); this describes any agitation, aggression, altered perception/thought content or escalated behaviours along with a diagnosis of dementia. Symptoms of BPSD can include disrupted thoughts, low mood/depression, altered perceptions or behaviours (such as agitation), psychosis, hallucinations, delusions and apathy (Dodd, et al., 2018). Each of the different symptoms is dependent on disease progression, and etiological factors, which manifest in biological, psychological and social ways (Byrne, et al., 2005). Of importance is the recognition that psychosis is no longer just related to schizophrenia. However, the profile of psychosis in dementia is significantly different from that seen in schizophrenia diagnosis (Leroi et al, 2003). As Zakrzewka-Sito and Kuczyńska (2021) point out, the reason psychosis is different in the elderly is that it is associated with dysregulation of the serotonergic system.
BPSD is commonly accompanied by a variety of difficult and sometimes challenging symptoms, including disturbed behaviour, thought, mood and perception, and poor impulse control (Buhagiar, et al., 2011). This results in health professionals or caregivers being challenged, and at times frustrated, when it comes to planning therapeutic interventions for their care. Consequently, when a patient with BPSD is labelled as aggressive, agitated and/or unmanageable, PRN antipsychotic medication is often administered without trying to implement nonpharmacological interventions such as redirection, or distraction. PRN antipsychotic medication is not recommended as a first-line intervention for managing challenging BPSD, and yet it is often used in this way. Overprescribing of PRN antipsychotics can result in over-sedation of patients, which creates greater risk of falls. According to Moniz-Cook et al (2001), although there is evidence to suggest that nonpharmacological interventions are best for individuals, using this as a first point of action for the treatment of BPSD is only occurring in limited areas of aged care. There is also the risk that personalised treatment plans and other nonpharmacological therapies will only work on occasion, as each patient presents differently and responds in different ways to treatment (Moniz-Cook et al). Due to the differences even within BPSD, one patient presenting with hallucinations/delusion will require completely different treatment from a patient presenting with agitation and sleep disturbance (Imtiaz et al, 2018).
This integrative review is a critique of research to determine the factors that make it challenging to use nonpharmacological interventions, thus leading to a reliance on PRN antipsychotics, in the care of individuals who have a diagnosis of dementia and present with BPSD.
METHOD
In 2005, Whittemore and Knafl developed the process of integrative review as a research methodology. It includes five stages: identify the problem of interest; search literature; evaluate literature; synthesise data; and finally, present data in a comprehensive and succinct way. An integrative review allows for a holistic approach by using various data sources for the research; in doing so, it enables a broader perspective of research that has been conducted on a specific topic (Whittemore & Knafl, 2005). Although this process may be structured in different ways, depending on the topic/review question and content, all integrative reviews are expected to follow a structured template (Melillo, 2020). Drawing on the principles of meta-analysis (Goldberg et al., 2022), a researcher creating an integrative review can synthesise data from multiple pieces of research, thus delivering a precise evaluation of the effectiveness of a single intervention (Conner, 2014).
The mnemonic PICO is a tool researchers can use to examine the phenomenon of interest; it is formulated as follows: population, intervention, comparison and outcomes (Cochrane Library, 2001). Using PICO ensures the data search remains focused and specific, which is important when completing the systematic portion of the review. The parameters for the search are detailed in Table 1 (below).
Table 1: PICO
| Population of interest | Older adults with dementia (45+ years)
A diagnosis of dementia with behavioural and psychological symptoms of dementia (BPSD) |
| Phenomenon of interest (intervention) | Use of PRN and the influencing factors in BPSD
Non-pharmacological approaches to BPSD |
| Context | People with dementia in aged residential care/acute settings requiring PRN medication |
However, for this study, rather than trying to “compare” (as specified in the PICO framework), the idea of “context” was used instead, as comparisons would not address the research question and were only apparent in some of the included articles. Search terms included (and were limited to): “older adults”, “behavioural and psychological symptoms of dementia”, “BPSD”, “behaviour management plans”, “acute care” and “aged residential care”. A 10-year date range was specified for articles to be accepted into the review. The only exception was the article by Crombie et al (2008), as its findings were particularly relevant to this review. The inclusion and exclusion criteria are summarised in Table 2 (below).
Table 2: Study inclusion and exclusion criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
|
|
|
|
|
|
| Date limits: 2009-2012, 2012-2022 | 1989-2009 |
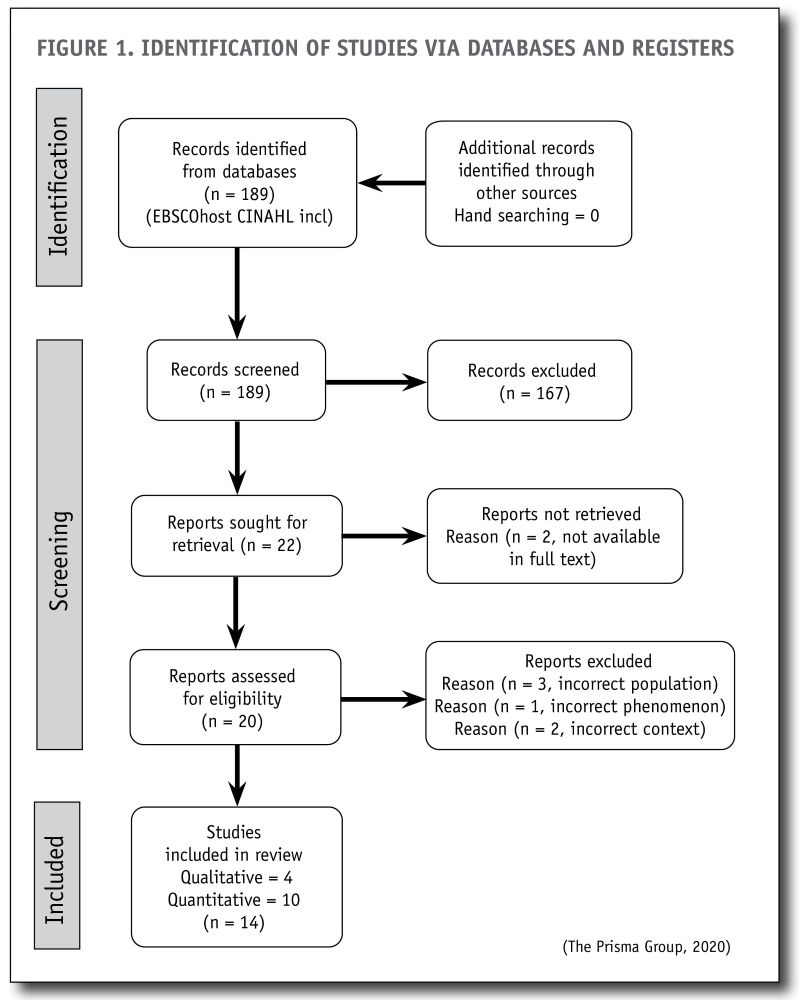
Using the specified search terms and inclusion/exclusion criteria, searches of databases revealed 189 potential articles for screening. The searches were recorded in a table, with the search strategy and study selection described using a Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) flow diagram (see Figure 1, below). This process resulted in 14 studies being selected for the review – four of them qualitative and 10 quantitative.
Data analysis is the essential process of an integrative review, synthesising diverse sources and facilitating better understanding of the issue being studied (Conner, 2014). For our analysis, each of the 14 articles was scrutinised and dissected to find its basic foundations, then evaluated and tabulated into structured form. In some literature, this process is called a “review matrix”, which is described as a way of extracting data from the relevant published research (Garrard, 2017). Table 3 (below) summarises how each article was assessed using the Joanna Briggs Institute (JBI) (Joanna Briggs Institute, 2020)appraisal for qualitative research, and also assessed for the strength of the evidence in accordance with guidelines developed by Ackley et al (2008).
Table 3: Level of evidence rating system
| Level of evidence (LOE) | Description |
|---|---|
| Level I | Evidence from a systematic review or meta-analysis of all relevant randomised controlled trials (RCTs) or evidence-based clinical practice guidelines based on systematic reviews of RCTs or three or more RCTs of good quality that have similar results. |
| Level II | Evidence obtained from at least one well-designed RCT (eg large multi-site RCT). |
| Level III | Evidence obtained from well-designed controlled trials without randomisation (ie quasi-experimental). |
| Level IV | Evidence from well-designed case-control or cohort studies. |
| Level V | Evidence from systematic reviews of descriptive and qualitative studies (meta-synthesis). |
| Level VI | Evidence from a single descriptive or qualitative study. |
| Level VII | Evidence from the opinion of authorities and/or reports of expert committees. |
Based on Ackley et al (2008)
The Ackley guidelines enable each article to be assessed in terms of how of the study design minimises the impact of bias on results. A Level I study (systematic review of randomised control trials) is considered the strongest level of evidence. Based on their study designs, the 14 studies chosen for this review were rated as follows: Level II, n = 1; Level III, n= 4; Level IV, n = 7; Level V, n=0, Level VI, n = 2.
The review matrix is presented below in Table 4.

FINDINGS
Three themes emerged from the review. The first finding was that low staff-to-patient ratios increased instances of challenging BPSD. The second finding was that the numbers of staff with specialised training were low suggesting the need to educate staff about the progression of dementia and/or the manifestation of BPSD, as well as the implementation of person-centred care plans. Lastly, it was found that using person-centred care plans reduced instances of BPSD.
Low staff-to-patient ratio
Studies from the UK (Backhouse et al, 2014), Germany (Richter et al, 2019) and Thailand (Lertkratoke et al, 2021) suggest that with populations ageing and more people being diagnosed with dementia and BPSD, there is pressure on aged residential care (ARC) facilities, which are already under strain. According to the Australian Institute of Health and Welfare (2015), 60 per cent of those diagnosed with dementia will be placed in ARC at some stage during their disease process. This is a concern because there are not enough beds, the staff-to-patient ratio is low, and the number of individuals entering ARC at high-level needs has been increasing since 2008 (New Zealand Nurses Organisation, 2012). It is not just a matter of low staff numbers, but low numbers of qualified/higher trained staff that the research has highlighted as a concern. Without adequate staff numbers to facilitate basic care for their patients, there is even less of a chance they can take extra time to implement a personalised plan to manage BPSD, therefore reducing PRN antipsychotic use (Brodaty & Low, 2003). Crombie et al. (2008) support this finding, reporting that staff shortages and an inability to manage BPSD effectively is a difficult situation to remedy as dementia facilities rely on additional funding and specific reviews to enable any change.
Skill set and the use of antipsychotic medications
In addition to low staffing levels, another issue in relation to overuse of anti-psychotics is a lack of appropriately trained staff (Roe et al, 2020). Roe et al pointed out that insufficiently skilled staff are unaware of the potential risks of frequently using (or overusing) psychotropic medication. Or they may lack the ability to distinguish the severity of the episode of BPSD they are faced with. Instead, the staff stated the individual was just “being difficult” or “not behaving“. What drives use of psychotropic medication may be the quantity of residents presenting with BPSD rather than the severity of the BPSD. For example, Carnahan et al (2017) report the use of antipsychotic drugs increased when the area was staffed more by nurse aides than when there was a registered nurse (RN) supervising care.
In some cases, while staff were willing to trial nonpharmacological interventions, there were gaps between their theoretical knowledge and their ability to put it into practice (Backhouse et al, 2016). Further education would be beneficial to encourage use of techniques such as de-escalation or distraction, which staff may be unaware of. To ensure the effectiveness of care plans, it is important staff are aware of the reasons behind nonpharmacological interventions, which requires further training. The principal author of this study notes from practice experience that just implementing such a document and expecting the staff to understand the desired outcome is short-sighted. Education becomes an essential aspect of this care and gives staff/caregivers the confidence to use person-centred care to help reduce the use of antipsychotic PRN medication.
Further training for staff
Training about the adverse effects of antipsychotic medication is imperative to reduce its use and encourage more nonpharma-
cological interventions. Understanding these medications, their mechanisms of action and their adverse effects are important aspects of care. Limiting their use also reduces the risk of over-sedation and falls. If this is not understood first, it is hard to expect staff to implement nonpharmacological interventions which are more work and take longer to show results (Roe et al, 2020).
Backhouse et al (2014) used postal surveys to obtain information about the management of BPSD, and concluded further staff training was imperative. They highlighted nonpharmacological interventions which aimed to both improve the individual’s quality of life by reducing their symptoms, and to ensure staff were less burdened. An example of the importance of the training can be found in the work of Lertkratoke et al (2021), who conducted research comparing two hospitals which promoted holistic care in areas with high prevalence of BPSD. They reported that nonpharmacological interventions were only available where staff were specialised in managing BPSD. However such specialised units had only limited capacity, meaning only 25 per cent of patients had access to this level of care. Following a 12-week programme of specialised training for staff caring for patients with BPSD, as in Ozakia et al (2017), the intervention group presented with significantly less caregiver burden than those in the comparison group.
Staff with the skills required for individualised assessment and intervention are infrequently found in care homes where multiple approaches are required to manage the complexity of care (Backhouse et al, 2016).
DISCUSSION
Nonpharmacological interventions such as person-centred care are recommended as a first-line intervention. However, this is rarely the case in practice (NICE and SCIE, 2006). The use of antipsychotic medication to reduce BPSD is still required at times. However, according to Saidlitz et al (2016), antipsychotic medication should only be used in the most severe cases and never as a first response to management. The use of person-centred care (Backhouse et al, 2016; Backhouse et al, 2014)) where facilities had put in place programmes that focused on the individual’s likes and dislikes was shown to be effective if the conditions were right. Small groups of residents were selected and observed for a trial which found that specific care plans were more effective in reducing BPSD. These researchers found it was important to try use of such plans more than once: Backhouse et al (2016) reported staff were required to “stick with it” when residents were unwilling to participate, or it appeared it wasn’t working. However, these authors acknowledged this did require skill and time.
According to Goodwin & Mangan (1985), the key to a successful individualised care plan is for staff to rid their thoughts of a “we/they” relationship with residents, turning instead to an “us” relationship. This message is still relevant 30 years after publication and remains best practice in this context. Gooodwin & Mangan’s (1985) message is that those living in care homes need to be treated more as equals who play an important role in their own care. This requires staff to look at who that person was prior to diagnosis – their hobbies, job, and what they enjoyed or disliked; all important and relevant information for staff. There is a phrase used among health professionals, “short-term pain for long-term gain”, which relates directly to the amount of work required to create and carry out a care plan individualised to the person. Resnick et al (2018) conducted their study by looking at the implementation of person-centred care to observe the correlation between care plans and care-plan checklists and any reduction of the symptoms of dementia. They found there is evidence to suggest care plans and care plan checklists are valid when caring for those with BPSD; however there was no direct link to reducing specific behaviours such as impulsivity, agitation and wandering. Further mentorship and motivation from senior staff did encourage the use of person-centred care plans, which is now the utilised first-line approach in long-term care settings (Resnick et al).
This approach is best found with research conducted by Honda et al (2016), who used a multimodal care approach called Humanitude. This approach, of French origin, is designed specifically for vulnerable older adults, and focuses on their emotions, communication and perceptions. These researchers used Humanitude in an acute-care hospital setting to assess its effect on BPSD. When this approach was compared to conventional care, a reduction was found in exhibited BPSD symptoms. Humanitude emphasises human emotion, with gentle touch, eye contact and verbal communication used in all interactions with patients in the study. It was found that in cases where the patient’s care was more complex or the symptoms more severe, it took longer for this approach to work and required more patience from staff. The other important outcome they found was a reduction in polypharmacy, which led to a reduction in the use of antipsychotics. Saidlitz et al (2016) examined specialised cognitive behaviour units in France which were created as part of that country’s Alzheimer Plan. The approach of these units to person-centred care was a combination of physical activity, relaxation, sensory and cognitive stimulation, and reorientation. These researchers examined the management of psychosocial behaviours (which they consider BPSD to fall under), and the effect it has on symptoms and the use of PRN antipsychotics as the first approach to care. Saidlitz et al (2016) found that using this style of management brought about a significant reduction in behavioural symptoms, particularly disruption to other patient care. There was an improvement in successful nonpharmacological interventions, leading to a reduction in antipsychotic use to treat behavioural issues.
As identified in this review by researchers including Honda et al (2016), Resnick et al (2018), Richter et al (2019) and Saidlitz et al (2016), facilities which used a “human” or individual approach found a decrease in problems with BPSD. Approaching a complex case by observing the whole person (including their past) reduces the risk of distress. This, along with appropriate humanistic cues, such as leading the individual by the hand to a room, ensures that the person feels safe, and is more likely to produce a positive response. Looking the person in the eye when speaking to them and talking to them in a clear and concise manner, gives the individual a better chance of understanding what the staff member is asking of them. Helping the person complete tasks rather than doing things to them, or for them, is the most important point to remember.
The fact that PRN medication is used more frequently than intended when prescribed raises issues about caring for those who present with BPSD. Ozaki et al (2017) suggested that clinicians are reluctant to use approaches other than pharmacological for fear of exacerbating BPSD behaviour. This is sometimes found to be a way for the staff to cope with what they feel is unmanageable or inappropriate behaviour and less about what might be sustainable long term. Learning how to manage clients using humanistic approaches is a skill that can be adapted to each individual’s situation. Using antipsychotic medication as an intervention in these circumstances carries a high risk of sedation and closes off the potential for individual interpersonal responses that may have greater therapeutic benefit in the long term.
LIMITATIONS
Most of the research selected for this review was based in European countries, the United States or Australia. With only three articles based in Asian countries, there was a strong western perspective on managing people affected by BPSD. A limitation of the study is that culturally responsive approaches to care were not specifically identified in the findings of the included studies.
RECOMMENDATIONS
Nursing staff who have completed advanced education in management of complex care/BPSD, and antipsychotic medications and their uses, have a more comprehensive understanding of BPSD and the reasons behind it. These staff are then able to create care plans individualised to the patient which, as seen in the articles reviewed, has a positive effect when conducted correctly, thus encouraging nonpharmacological interventions. These specialised staff are able to role-model this care for fellow staff and provide them with advice and support.
- To ensure individualised care plans are created and used correctly, it is important staff are educated specifically on person-centred behaviour management.
- To encourage ongoing education, using a specialist dementia care nurse (such as a clinical nurse specialist) who provides regular training programmes will give staff the confidence to continue with care plans.
CONCLUSION
BPSD is complex and difficult to manage, complicated by a mix of low staffing, and/or inadequate training opportunities. As the research in this review shows, more training about BPSD and the risks of antipsychotic medication, paired with the use of nonpharmacological care plans, can reduce symptoms. These approaches can ultimately reduce the use of antipsychotic medication as a first response. Having staff in aged-care facilities with specialist knowledge benefits the entire institution. The reduction in BPSD has a ripple effect from the staff who care for these patients, to the management who don’t need to find alternative care or deal with burnt-out staff.
REFERENCES
Ackley, B., Swan, B., Ladwig, G., & Tucker, S. (2008). Finding and Evaluating Research in Practice. In B. Ackley, Evidence-based nursing care guidelines: Medical-surgical interventions (p. 7). Mosby Elsevier.
Australian Government. (2015). Australia’s welfare 2015 in brief. Australian Institute of Health and Welfare.
Backhouse, T., Killet, A., Penhale, B., & Gray, R. (2016). The use of non-pharmacological interventions for dementia behaviours in care homes: findings from four in-depth, ethnographic case studies. Age and Ageing, 856-63.
Backhouse, T., Killet, A., Penhale, B., Burns, D., & Gray, R. (2014). Behavioural and psychological symptoms of dementia and their management in care homes within the East of England: a postal survey. Ageing and Mental Health, 18(2), 187-93.
Brodaty, H., & Low, L.-F. (2003). Aggression in the elderly. Journal of Clinical Psychiatry, 64, 36-43.
Buhagiar, K., Afzal, N., & Cosgrave, M. (2011). Behavioural and psychological symptoms of dementia in primary care: a survey of general practitioners in Ireland. Mental Health in Family Medicine, 227-234.
Byrne, E., Robert, P., Verhey, F., Hurt, C., De Deyn, P., Nobili, F., & Vellas, B. (2005). Grouping for behavioral and psychological symptoms in dementia: Clinical and biological aspects. European Psychiatry, 20, 490-496.
Carnahan, R., Brown, G., Letuchy, E., Rubenstein, L., Gryzlak, B., Reist, J., Kelly, M., Schultze, S., Weckmanne, M., & Chrischilles, E. (2017). Impact of programs to reduce antipsychotic and anticholinergic use in nursing homes. Alzheimer’s & Dementia: Translational Research & Clinical Interventions, 3, 553-561.
Cloak, N., & Al Khalili, Y. (2022). Behavioral And Psychological Symptoms In Dementia. StatPearls Publishing.
Cochrane Library. (2001). Cochrane PICO search.
Conner, B. (2014). Demystifying literature reviews. American Nurse Today, 9(1), 13-14.
Crombie, A., Snell, T., & Boyd, J. (2008). The ABC of managing behavioural and psychological symptoms of dementia. Geriaction, 26(2), 14-24.
Dodd, K., Watchman, K., Janicki, M., Coppus, A., Gaertner, C., Fortea, J., Santosi, F., Kelle, S., & Strydom, A. (2018). Consensus statement of the international summit on intellectual disability and dementia related to post-diagnostic support. Aging & Mental Health, 22(11), 1406-1415.
Duong, S., Yeung, K.-T., & Chang, F. (2015). Intramuscular olanzapine in the management of behavioral and psychological symptoms in hospitalized older adults: a retrospective descriptive study. Journal of Aging Research.
Garrard, J. (2017). Review matrix folder: How to abstract the research literature. In J. Garrard, Health sciences literature review made easy: The matrix method (pp. 119-138). Jones & Bartlett Learning.
Goldberg, J., Boyce, L., Soudant, C., & Godwin, K. (2022). Assessing journal author guidelines for systematic reviews and meta-analyses: Findings from an institutional sample. Journal of Medical Library Association, 110(1), 63-71.
Goodwin, S., & Mangan, P. (1985). Cosmic nursing: do old people come from outer space? Nursing Times, 81(28), 52-53.
Honda, M. I., Ito, M., Ishikawa, S., Takebayashi, Y., & Tierney Jr, L. (2016). Reduction of behavioral psychological symptoms of dementia by multimodal comprehensive care for vulnerable geriatric patients in an acute care hospital: A case series. Case Reports in Medicine.
Imtiaz, D., Khan, A., & Seelye, A. (2018). A mobile multimedia reminiscence therapy application to reduce Behavioral and Psychological Symptoms in persons with Alzheimer’s. Journal of Healthcare Engineering, 1-9.
Joanna Briggs Institute. (2020). Critical appraisal checklist for qualitative research.
Leroi, I., Voulgari, A., Breitner, J., & Lyketsos, C. G. (2003). The epidemiology of psychosis in dementia. American Journal of Geriatric Psychiatry, 11(1), 83-91.
Lertkratoke, S., Amnatsatsue, K., Kerdmongkol, P., & Nanthamongkolchai, S. (2021). Effectiveness of Thai integrated care program for older adults with dementia in the community: a quasi-experimental study. Pacific Rim International Journal of Nursing Research, 25(4), 510-524.
Mallon, C., Krska, J., & Gammie, S. (2019). Views and experiences of care home staff on managing behaviours that challenge in dementia: A national survey in England. Aging & Mental Health, 23(6), 698-705.
Manso-Calderon, R., Cacabelos-Perez, P., Sevillano-Garcia, M., Herrero-Prieto, M. E., & Gonzalez-Sarmiento, R. (2020). The impact of vascular burden on behavioural and psychological symptoms in older adults with dementia: The BEVASDE study. Neurological Sciences, 41, 165-174.
Melillo, K. (2020). Formulating Review Question. In C. E. Toronto & R. Remington, A Step-By-Step Guide to Conducting an Integrative Review (pp. 13-14). Springer International Publishing.
Moniz-Cook, E. W., Woods, R. T., & Richards, K. (2001). Functional analysis of challenging behavior in dementia: The role of superstition. International Journal of Geriatric Psychiatry, 16, 45-56.
New Zealand Nurses Organisation. (2012). NZNO Research policies that can transform healthcare: Mandated nursing staff to resident ratios in aged care: Summary of evidence.
NICE and SCIE. (2006). Dementia: supporting people with dementia and their carers in health and social care.
Ozakia, T., Katsumata, Y., & Arai, A. (2017). The use of psychotropic drugs for behavioral and psychological symptoms of dementia among residents in long-term care facilities in Japan. Aging & Mental Health, 21(12), 1248-1255.
Resnick, B., Galik, E., Kolanowski, A., Van Haitsma, K., Ellis, J., Behrens, L., Flanagan, N., & McDermott, C. (2018). Reliability and validity of the care plan checklist for evidence of person-centered approaches for behavioral and psychological symptoms associated with dementia. Journal of the American Medical Directors Association, 19, 613-618.
Richter, C., Berg, A., Langner, H., Meyer, G., Köpke, S., Balzer, K., Wolschon, E. M., Silies, K., Sönnichsen, A., Löscher, S., Haastert, B., Icks, A., Wolf, U., & Fleischer, S. (2019). Effect of person-centered care on antipsychotic drug use in nursing homes (EPCentCare): a cluster-randomised controlled trial. Age and Ageing, 48, 419-425.
Roe, J. C., Coulson, S., Ockerby, C., & Hutchinson, A. M. (2020). Staff perceptions of caring for people exhibiting behavioural and psychological symptoms of dementia in residential aged care: A cross-sectional survey. Australian Journal on Ageing, 39, 237-243.
Saidlitz, P., Sourdet, S., Voisin, T., & Vellas, B. (2016). Management of behavioural symptoms of dementia in a specialized unit care. Psychogeriatrics, 17, 81-88.
BMJ. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews.
Whittemore, R. &. Knafl, K. (2005). The integrative review: updated methodology. Journal of Advanced Nursing, 52, 546-553.
Zakrzewska-Sito, A., & Kuczyńska, J. (2021). Searching for new drugs for the treatment of dementia-related psychosis. Postepy psychiatrii neurologii, 30(4), 270-277.
Daily doses – uncut news
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


