
About the authors:Chris Moir, RN, PhD, GradCertTertT, is a senior lecturer at the Centre for Postgraduate Nursing Studies, University of Otago, Christchurch. Maria Baby, RN, MHSc, PhD, is a clinical nurse specialist in the intellectual disability service, Te Whatu Ora – Southern, Dunedin. This article was accepted for publication in September 2022. |
ABSTRACTBackground: Violence and aggression toward nurses are workplace hazards that have been exacerbated by the Covid-19 pandemic. In clinical practice placements, nursing students sometimes bear the brunt of aggression from both patients and staff. The skills to respond safely and appropriately to these workplace hazards should be taught before students undertake clinical practice experiences. Therefore, teaching de-escalation skills early in the nursing programme is vital for student safety, and perhaps ultimately for their retention in the nursing workforce. Objectives: To determine the effectiveness of early communication skills training to enhance nursing students’ aggression management skills while on clinical placement. Design: A quasi-experimental design using pre- and post-tests of communication competence following an education module delivered as part of the curriculum. Sample and setting: Participants were students in a master of nursing science pre-registration programme. Methods: Thackrey’s Confidence in Coping with Patient Aggression Instrument and the Interpersonal Communication Competence Scale were administered at baseline before the communication session was taught. The same questionnaires were administered after the participants had completed clinical placements in acute care and mental health. Results: There were 33 nursing student participants. Outcome measures indicated a significant increase in both aspects of communication confidence and competence from baseline across the two placements for the combined cohorts. Conclusion: The study highlights the need to deliver communication skills training early in the nursing programme to enable nursing students to develop confidence in dealing with aggression across all areas of health care. |
||
KEYWORDSGEN students, aggression, violence, communication skills, clinical placement, education |
|||


INTRODUCTION
THE IMPETUS FOR THIS research was a poster on a board outside a ward nurses’ office, alerting people to the fact that “No abuse of staff will be tolerated”. This led to consideration about what content in the nursing curriculum prepared students to respond appropriately to violence or aggression in general wards. Since then, many such posters have been observed in all environments where nurses work, and violence in the health workplace has become more commonly discussed. During the COVID-19 pandemic, government measures to control the disease inspired strong emotions in some members of the public – the Wellington protests at the extreme end – and caused increased friction between the public and health workers. This recent evidence of the potential for health staff to become inadvertently involved in such conflict, shows that the notion of embedding aggression management in pre-registration nursing education is timely (Dyer, 2021).
Workplace violence has been reported throughout the health service (International Labour Office, International Council of Nurses, World Health Organization, and Public Services International, 2002; WorkSafe New Zealand, 2016). It is considered a serious occupational hazard facing personnel working in today’s health-care environment (Duxbury & Whittington, 2005; Hahn et al., 2012; Shafran-Tikva et al., 2017; Winstanley & Whittington, 2004). The United States (US) Occupational Safety and Health Administration defines workplace violence as “any act or threat of physical violence, harassment, intimidation or other threatening disruptive behaviour that occurs at the work site.” (OSHA, 2016). According to the US National Institute of Occupational Safety and Health (2021), workplace violence typically falls into one of four categories: Type I – criminal intent, Type II – patient/client, Type III – worker on worker and Type IV – personal relationship. Type II and Type III are particularly relevant to nursing students, who have less experience with clients in the workforce to draw on (Minton et al., 2018; Nowrouzki-Kia et al., 2019).
BACKGROUND
Nursing students are likely to encounter aggressive behaviour during clinical placements (Jackson et al., 2011; Magnavita & Heponiemi, 2011; Hopkins et al., 2014; Heckemann et al., 2015). For the purpose of this study, violence was defined as “any form of verbal or physical threat or assault perpetrated by patients towards the student nurse” (Type II). It excludes other forms of violence which include bullying by family or other clinicians as perpetrators of aggression/violence.
A recent study on medical and nursing students’ experience of violence in clinical placements noted over half the students reported having experienced verbal violence during their placements (Warshawski, 2021). This is a disturbing figure. Nursing students are at high risk of being victims of various types of aggression, ranging from verbal aggression to physical assault (Nau et al., 2009; Jackson et al., 2011; Magnavita & Heponiemi, 2011). Inexperience and lack of training, and younger age, have been identified as possible risk factors (Nau et al., 2011; Magnavita & Heponiemi, 2011; Hopkins et al., 2014; Brann & Hartley, 2017). Exposure to such behaviour could have a detrimental effect on their professional identity, values and attitudes if adequate preparation and support are not offered early in their education (Hopkins et al., 2014; Jeong & Lee, 2020; Warshawski, 2021).
In New Zealand, aggression management training is available and mandated as part of working in areas identified with potential for aggression and violence (Swain et al., 2014; Te Pou, 2016). The currently mandated training for all staff working in inpatient mental health services in district health boards (DHBs)1 in New Zealand is the Safe Practice Effective Communication training. This is a four-day DHB-based national training course which teaches best and least restrictive practice in mental health inpatient units. This includes training in restraint minimisation, communication, de-escalation and collaboration, and personal restraint and breakaway techniques (Te Pou, 2016). However, this training is limited to the qualified workforce employed by DHBs.
Aggression management is an important issue for nursing students that requires attention during education before they undertake clinical practice. While evidence exists of the effectiveness of communication skills training for registered nurses (RNs) and health-care assistants such as the Workplace Violence Prevention Training Program intervention (Story et al., 2020), and “It’s all about communication” (Baby et al., 2018), there is minimal evidence of the effectiveness of incorporating such training early in the education of health-care workers. De-escalation is commonly a component of mental health education. While some nurse education programmes place mental health early in the programme, others have it later. Given the apparent ubiquity of violence towards nursing students while on placements, the advent of a mental health placement should not determine the placement of this training as it appears it is necessary earlier, as part of therapeutic relationship education. For this reason, determining the communication styles of students and providing strategies/interventions to prevent, minimise and prepare them to cope and manage exposure to aggression in clinical placements would be beneficial at an early stage of their education programme (Bilgin et al., 2016; Hopkins et al., 2018; Heckemann et al., 2015).
This study aimed to assess the effectiveness of an aggression prevention and minimisation education package, “It’s all about communication”, for graduate-entry nursing students in guiding their coping with aggressive situations during clinical placements.
METHODS
Design
This is a quasi-experimental study, which uses a pre-test/post-test design to evaluate the effectiveness of a communications skills training programme for graduate nursing students to help them cope with aggression and violence during clinical placements. In this design, baseline measurements were compared with equivalent measurements made after the delivery of the educational intervention, post two clinical placements (acute care and mental health), to assess any change in the outcome variables that the intervention was designed to influence. The training was delivered as part of the standard curriculum for a master of nursing science programme. All students attended the education session, irrespective of their participation in this research study.
Setting and sample
The participants were nursing students in the first year of a graduate-entry master of nursing science programme at a New Zealand university in 2019 and 2020. This programme is an intensive integrated course of study, usually completed in two full-time years, which offers a pathway to a nursing career for graduates of any discipline.
Head of school approval was obtained for this study as part of the University of Otago ethical approval process. The principal investigator (CM) is the clinical coordinator for the master of nursing science and teaches students and assesses them in clinical placements. Therefore, the issue of coercion of students to participate was considered in the planning of this study. To avoid potential coercion, the students were given an information sheet before the consenting process. This explained that all completed questionnaires would be de-identified, that participation in the study was optional, and not participating would have no negative effects on their progression through the course. Co-researcher MB delivered the education package to both cohorts to ensure consistency in teaching. All surveys were directed to an administrator for de-identification before the data was entered into spreadsheets.
Intervention
The training module, “It’s all about communication”, was developed by Swain and Gale (2014) as an intervention for community support workers in New Zealand, to help them manage patient aggression. It was piloted and trialled as a randomised controlled trial (RCT) with promising results (Baby et al., 2018; Swain & Gale, 2014). The content of the communication skills package is derived from skills listed in the Calgary Cambridge Model of Communication teaching and learning in medicine (Silverman et al., 2013) and based on experience teaching communication skills to medical students. The sessions are structured from basic to complex. It involves pairwise and group discussions for each of the components. Examples on DVD were enacted by professional actors – these videos were based on true clinical situations which had been de-identified and modified to ensure privacy. The four sessions included communication techniques, working in groups, difficult situations and when to move on (see Table 1, below).
Table 1: Outline of ‘It’s all about communication’ training
Communication techniques
|
Working in groups
|
Difficult situations
|
When to move on
|
Data collection and outcome measures
The educational intervention “It’s all about communication” was delivered as part of the first-year communication component in October 2019 to the 2019 cohort, and in March 2020 to the 2020 cohort. Written informed consent was obtained from those agreeing to participate in the research study before the teaching session. A purpose-designed questionnaire was used to collect demographic information from the participants, and data on their confidence in coping with patient aggression and self-assessed communication competence at three time points:
(i) before the education session, as baseline,
(ii) after the acute care placement and,
(iii) after the mental health placement.
The nursing students completed five weeks of clinical placement in acute care settings (the 2019 cohort in November/December 2019, and the 2020 cohort in November/December 2020) and five weeks in mental health settings (the 2019 cohort in February/March 2020 and the 2020 cohort in February/March 2021). Following each placement, participants completed questionnaires which had been sent to their academic nurse supervisor. Students were asked to complete the questionnaire after their summative assessment interview. These were collected by the academic supervisor and sent to the administrator for de-identification. It is important to note that students’ normal course content for their mental health placement included personal safety and de-escalation sessions, so this intervention brought them additional de-escalation teaching before their mental health placement.
The demographic section of the questionnaire gathered information about the participants’ gender, ethnicity, age, basic and health-care specific educational qualifications, health-care work experience and previous aggression management and communication skills training.
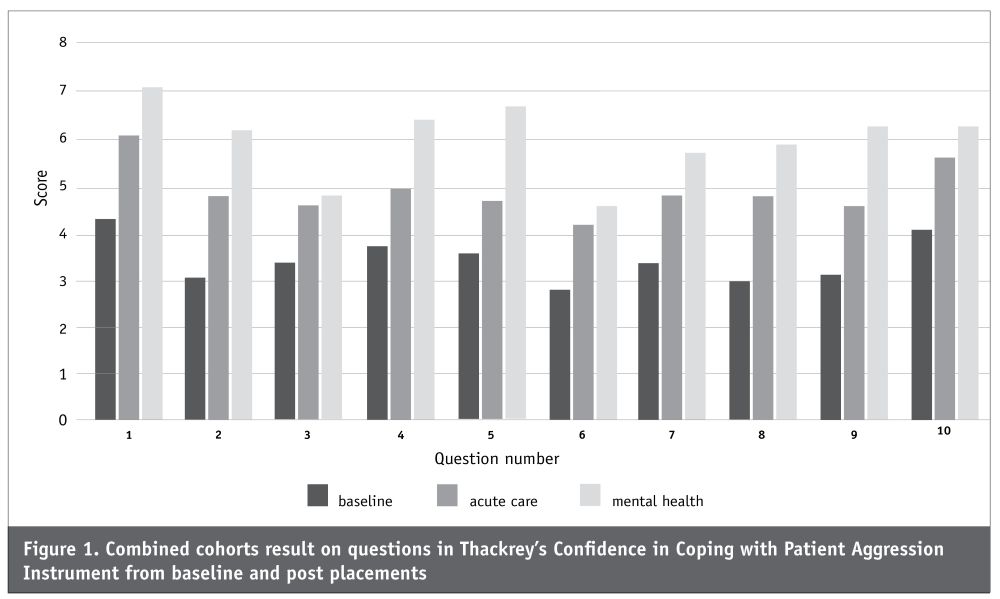
Confidence in coping with patient aggression was measured with the scale developed by Thackrey in 1987 (Thackrey’s Confidence in Coping with Patient Aggression Instrument). The instrument consists of 10 items rated on an 11-point scale from least confident to very confident. A high score indicates strong confidence in dealing with patient aggression. This scale has been found to be a useful instrument for evaluations of groups when used as a pre-test/post-test measure (Guay et al, 2016; Nau et al, 2011).
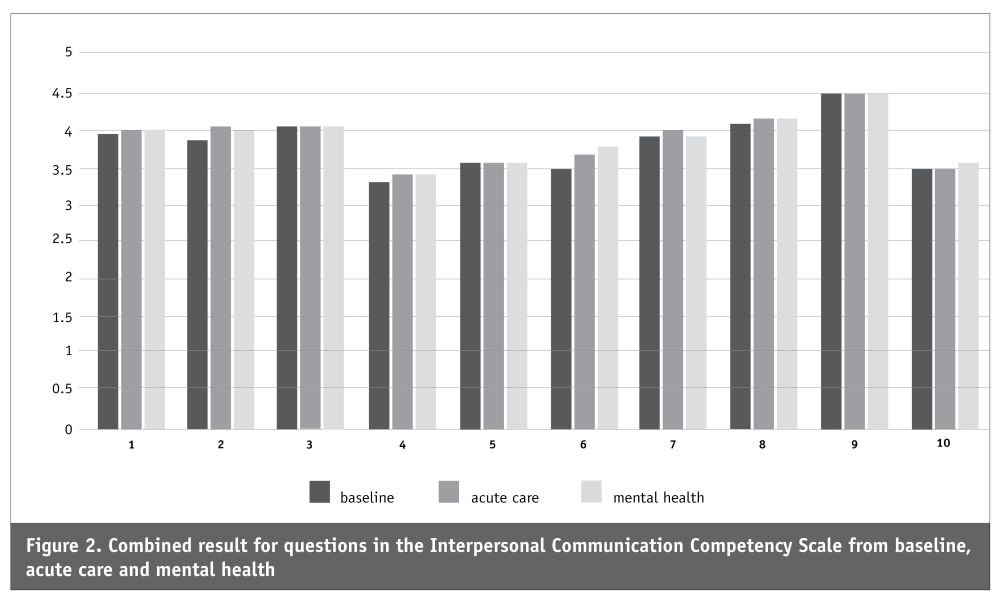
Competence in interpersonal communication is an impression or judgment formed about a person’s ability to communicate in interpersonal relationships. The Interpersonal Communication Competence Scale is a brief, self-report measure of 10 interpersonal communication competence skills, which include self-disclosure, empathy, social relaxation, assertiveness, interaction management, altercentrism, expressiveness, supportiveness, immediacy and environmental control (Rubin & Martin, 1994). Each of the items are scored as 5 = almost always, 4 = often, 3 = sometimes, 2 = seldom and 1 = almost never. The scores range from 30 to 150, with higher scores indicating positive results. The 30-item scale has an overall alpha of 0.86, showing internal reliability and strong concurrent validity (Rubin & Martin, 1994). This scale is strongly related to cognitive and communication flexibility and is suitable for measuring communication skills among health-care workers/trainees (Ang, Swain, & Gale, 2013).
An open question, included in the questionnaires which followed each of the two clinical placements, provided an opportunity for participants to comment on their application of teaching from “It’s all about communication” in the clinical environment. Participants were asked: “Please tell us about any situation in your clinical placement where you felt you were specifically aware of applying the teaching from ‘It’s all about communication’ sessions. In doing so, please ensure the confidentiality of patient information by using pseudonyms and omitting any specific content which could identify an individual.”
Data analysis
The data was analysed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 27) and using an alpha of 0.05. Descriptive statistics were used in the presentation of the demographic variable of the two cohorts and the total of both cohorts. Paired sample t-tests were performed on continuous data to estimate the differences in participants’ scores between the pre-test (T1) and the two post-tests (T2 and T3) for the two outcomes scales, measuring confidence in coping with patient aggression and interpersonal communication competence. Feedback from the open question about the practical application of the intervention is presented as a summary from each placement.
Ethical considerations
Ethical approval was obtained from the University Human Ethics Committee before starting the study (19/124). The participants received an information sheet detailing the purpose of the study. Given the nature of the questionnaire, information could be sensitive, so questionnaires were de-identified before they were given to the researchers. Students were given a number to record on their questionnaire which was their participant number for all analysis. The master of nursing science administrator held the coding list and ensured that the questionnaires were coded correctly. Also, participants were given sufficient time to allow them to reflect on the implications of participation and not feel pressurised into taking part, despite the intervention being delivered as part of the curriculum. The research did not receive any grant funding from agencies in the public, commercial, or not-for-profit sectors.
RESULTS
Over the course of 2019 and 2020, 33 master of nursing science students participated in this study. Twelve were from the 2019 cohort and 21 from the 2020 cohort. Table 2 (below) outlines details of the demographic variables considered.
Table 2: Demographic details of the two cohorts
| Cohort | 2019 (n=12) |
2020 (n=21) |
Frequency | |
|---|---|---|---|---|
| N (n=33) | % | |||
| Gender | ||||
|
• Male • Female |
1 11 |
1 20 |
2 31 |
6 94 |
| Ethnicity | ||||
|
• NZ European • Other |
9 3 |
13 8 |
22 11 |
67 33 |
| Age | ||||
|
• Under 25 • 25-34 • 35-44 • 45-54 |
9 1 1 1 |
13 5 1 2 |
22 6 2 3 |
66 18 6 9 |
| Experience working in health care | ||||
|
• Yes • No |
1 11 |
8 4 |
10 11 |
55 45 |
| Highest qualification | ||||
|
• Bachelor’s degree • Master’s degree • PG diploma |
11 1 0 |
16 3 2 |
27 4 2 |
81 12 6 |
| Previous aggression management training | ||||
|
• Yes • No |
2 10 |
2 19 |
4 29 |
12 88 |
Ethnicities with less than three people are reported as “other” to maintain anonymity. The majority of students (67 per cent) were NZ European, under 25 years old, with a bachelor’s degree, and around half (55 per cent) had work experience in a health-care setting. A few (n=4) had previous training in working in aggressive situations. Three students did not complete all three questionnaires, one from the 2019 cohort (who did not complete the acute care questionnaire) and two from the 2020 cohort (who did not complete the mental health questionnaire). The total number of questionnaires in the data was adjusted accordingly. The questionnaires they did complete were still included in the data for analysis.
Table 3 (below) indicates confidence in coping with patient aggression during clinical placements increased across all the 10 items on the CCPA measure for the 2020 cohort.
Table 3: Cohort results on Thackrey’s Confidence in Coping with Patient Aggression Instrument (CCPA) for baselines and two placements
| Baseline | Baseline | Acute care |
Acute care |
Mental health |
Mental health |
|
|---|---|---|---|---|---|---|
| Timeline and cohorts | 2019 m(SD) |
2020 m(SD) |
2019 m(SD) |
2020 m(SD) |
2019 m(SD) |
2020 m(SD) |
|
4.50 (1.45) |
4.05 (1.88) |
6.91 (2.02) |
5.58 (2.12) |
7.36 (1.20) |
7.00 (1.37) |
|
2.92 (1.78) |
3.05 (1.79) |
5.64 (1.69) |
4.26 (2.32) |
5.83 (1.89) |
6.42 (1.84) |
|
3.17 (1.64) |
3.30 (2.79) |
5.27 (1.61) |
4.19 (2.71) |
4.25 (2.05) |
5.16 (2.71) |
|
3.75 (2.05) |
3.65 (1.95) |
6.00 (1.94) |
4.43 (2.25) |
6.75 (1.42) |
6.21 (1.75) |
|
3.00 (1.76) |
3.75 (1.83) |
5.18 (1.60) |
4.62 (2.06) |
6.92 (1.08) |
6.37 (1.60) |
|
2.67 (1.92) |
2.95 (2.52) |
5.09 (2.21) |
3.95 (2.35) |
4.00 (1.95) |
4.95 (2.35) |
|
3.25 (1.42) |
3.30 (1.86) |
5.65 (2.16) |
4.57 (2.09) |
5.67 (2.19) |
5.79 (2.02) |
|
3.00 (2.00) |
3.05 (1.83) |
5.73 (2.28) |
4.42 (2.41) |
6.00 (2.10) |
5.74 (2.32) |
|
3.33 (1.61) |
3.05 (1.76) |
5.27 (1.62) |
4.38 (1.99) |
6.25 (1.60) |
6.37 (1.57) |
|
4.08 (1.38) |
3.95 (2.66) |
6.36 (2.84) |
5.14 (2.52) |
5.92 (2.39) |
6.53 (2.17) |
| Total scale score | 3.36 (1.40) |
3.40 (1.93) |
5.71 (1.78) |
4.65 (2.10) |
5.90 (1.15) |
6.06 (1.68) |
On the 11-point scale at baseline, the mean score of 2 to 4 indicates participants had a relatively low level of confidence. After two placements, the scores of 6 and 7 indicate an increase to medium level of confidence. Examining the results by individual question, there was a drop in mean scores relating to physically intervening with aggressive patients, level of training for handling physical aggression, and ability to protect self from an aggressive patient in the 2019 cohort between acute care and mental health placements (range of drop 0.44-1.02). As this was the smaller cohort, these results did not influence significance in outcomes for the combined group. Analysis of within-subjects changes (combined cohorts) of total scores across time using paired samples t-tests indicated a statistically significant increase in confidence coping with patient aggression as the students progressed through placements. The shift in confidence in coping with patient aggression between baseline and mental health (mean (SD) of -24.9(14.10), t=9.867, df=29, p=0.000) shows this. There was a statistically significant increase reported between acute care and mental health, with a mean (SD) = -9.07(14.69), (t=3.324, df=28, p=0.0).
Figure 1 (below) illustrates the increase in confidence across placements for the combined cohorts; confidence increased for each question in the questionnaire.
Results for the Interpersonal Communication Competence Scale (ICCS) show an increase in competence reported by the participants across times.
Table 4: Group comparison of Interpersonal Communication Competency Scale (ICCS) results for two cohorts at baseline and across two placements
| ICCS item | Baseline 2019 m(SD) |
Baseline 2020 m(SD) |
Acute care 2019 m(SD) |
Acute care 2020 m(SD) |
Mental health 2019 m(SD) |
Mental health 2020 m(SD) |
|---|---|---|---|---|---|---|
| 1. Self-disclosure | 3.86 (0.64) |
3.84 (0.79) |
4.06 (0.57) |
4.00 (0.68) |
4.03 (0.69) |
4.02 (0.70) |
| 2. Empathy | 3.75 (0.45) |
3.78 (0.40) |
4.03 (0.28) |
4.09 (0.46) |
4.12 (0.37) |
3.98 (0.53) |
| 3. Social relaxation | 4.11 (0.36) |
4.02 (0.55) |
4.21 (0.37) |
4.00 (0.72) |
4.25 (0.59) |
3.96 (0.59) |
| 4. Assertiveness | 3.08 (0.59) |
3.48 (0.75) |
3.30 (0.66) |
3.47 (0.61) |
3.31 (0.16) |
3.47 (0.68) |
| 5. Altercentrism | 3.67 (0.28) |
3.48 (0.23) |
3.55 (0.31) |
3.58 (0.30) |
3.64 (0.46) |
3.53 (0.47) |
| 6. Interaction management | 3.36 (0.44) |
3.59 (0.49) |
3.67 (0.37) |
3.67 (0.55) |
3.78 (0.30) |
3.81 (0.36) |
| 7. Expressiveness | 3.75 (0.77) |
3.95 (0.63) |
3.97 (0.43) |
4.10 (0.50) |
4.03 (0.50) |
3.81 (0.66) |
| 8. Supportiveness | 4.22 (0.48) |
4.13 (0.45) |
4.36 (0.31) |
4.18 (0.51) |
4.30 (0.52) |
4.20 (0.48) |
| 9. Immediacy | 4.47 (0.44) |
4.48 (0.51) |
4.55 (0.22) |
4.46 (0.52) |
4.53 (0.36) |
4.40 (0.63) |
| 10. Environmental control | 3.52 (0.41) |
3.41 (0.58) |
3.45 (0.52) |
3.58 (0.49) |
3.67 (0.49) |
3.63 (0.43) |
| Total score | 113.42 (6.64) |
114.19 (8.66) |
117.45 (7.60) |
116.94 (9.80) |
118.00 (8.83) |
114.81 (10.22) |
At baseline, the mean (SD) of 113.91(7.89) increased to 117.15(8.81) for acute care, followed by a slight drop in total mean (SD) at mental health of 116.11(9.64), an overall increase of 2.2 on the total score. There was a significant difference in the scores for baseline and after the acute-care placement, (t=2.74, df=26, p=0.01). A similar statistically significant improvement in competence in communication was evident between baseline and mental health (t=2.05, df = 26, p=0.05). However, the changes in communication competence between clinical placements (acute care and mental health) were not significant. The lowest scores were recorded for 4. Assertiveness (“standing up for one’s rights without denying the rights of the other”) and 10. Environmental control (“demonstrating one’s ability to achieve predetermined goals and satisfy need”). Consistently, the highest score was for 9. Immediacy which the authors of the ICCS describe as “showing others that you are approachable and available for communication” (Rubin & Martin, 1994, pp. 35-37). While the total scores showed a significant increase from baseline to each placement, Figure 2 (below) illustrates that this was mainly from an increase in four questions, rather than consistently across the questionnaire.
The summary of the responses from the open question on the practical application of the education session shows students’ comments made after acute-care placements were likely to be about communication with nurses and other members of the health-care team. The comments after mental health placements were more focused on communication with patients (see Table 5, below).
Table 5: Summary of open question feedback of practical implications of the educational intervention “It’s all about communication’
| Area of placement | Feedback/comments |
|---|---|
| Acute care |
|
| Mental health |
|
DISCUSSION
This study involved delivering an educational intervention to students in the early stages of their nursing education to increase their communication and de-escalation skills. The aim was to adequately equip them to manage aggression, given that research indicates they can experience this in all placements and from a variety of sources (Hallet et al., 2021; Heckemann et al., 2015; Hopkins et al., 2014; Jackson et al., 2011; Magnavita & Heponiemi, 2011). For the first of two measures, Thackrey’s Confidence in Coping with Patient Aggression scale indicated that for the students in the 2020 cohort, confidence increased for all 10 items across clinical placements. However in the 2019 cohort, the confidence scores were noted to decrease from acute care to mental health placement on three items of the scale dealing with physical aggression (items 3, 6 &10). It may be that the greater number of participants in 2020 reduced the variation, as the combined group change was significant.
However, it is also plausible that post mental health placements, students had been challenged and realised their confidence in dealing with physical aggression was lower. Thackrey’s scale has previously been used after teaching sessions on aggression management with registered nurses (RNs). Story et al. (2020) reported a pre-training mean of 55.1, indicating a higher baseline mean than this group of students (33.8); they report the post-training mean as 78.8, a mean increase of 23.7 (43 per cent). The present study reports an increase in mean of 26.12 from baseline to the mental health placement (60.00), an increase of 77 per cent. Most of this increase was evident between baseline and acute care placements, where the post result was 50.3, a 48 per cent increase.
Although the majority of the students in this study had previous experience in other roles in health care, the years of nursing experience reported in the study conducted by Story et al. (2020) was six to 10 years. Story et al (2020) used items 1 and 4 as pertinent questions in analysis of their results with their RN participants. They found around a 24 per cent increase from pre- to post-training for those questions on perceptions of comfort and confidence in dealing with patient aggression. This current study showed increases on those questions of 67 per cent and 71 per cent respectively, indicating a high level of increase in comfort and confidence among participants. This finding could be due to increased confidence in dealing with consumers of care in the clinical setting across placements as a result of the training, and also due to experiential learning. The current study’s student participant group may have set a benchmark for student cohorts using Thackrey’s scale which other studies might use for comparison. This also highlights that students have lower levels of confidence in managing/facing aggression in clinical settings than experienced RNs, and a targeted intervention such as the communication skills training programme delivered within the early stages of education appears to be beneficial.
For the second measure used, the Interpersonal Communication Competence Scale, another research study with a student cohort makes a useful comparison. The participants in an Australian study – a group of paramedical students – had similarities to the cohort in this study (Ross et al., 2014). Similarities in the age of participants across both studies is noted, with 86 per cent less than 26 years of age. The results in the comparative study indicated students were more confident in their communication across the aspects of empathy, supportiveness and immediacy (Ross et al., 2014). At baseline, the participants in the current study also rated themselves the highest on supportiveness and immediacy. However, the lowest scores were for assertiveness, which remained the lowest scoring aspect in the outcome measure across all three time points. This is concerning, given this is a group of graduate students who might be expected to have similar level of assertiveness to the cohort of paramedical students represented in the study by Ross et al. (2014). Given that 40 per cent of a group of New Zealand undergraduate nursing students reported worker-on-worker bullying in their clinical placements (Minton et al., 2018), assertiveness training could also be a useful addition to pre-registration nursing education. The highest score for “immediacy” – defined as “showing others that you are approachable and available for communication” – is consistent with the communication style associated with nursing and the caring professions in general.
The students’ increased confidence with communication was supported by the comments in the open questions. The open questions also allowed the researchers to determine which specific components of the educational intervention had practical applicability for students in their clinical placements. Students’ responses indicated they considered patients/family and co-workers in their application of the communication teaching. Given two out of four types of workplace violence classification include Type II (patient/client) and Type III (worker on worker), the comments of the nursing students indicate they are thinking broadly of the definition of this phenomenon, and the practical application of the education intervention.
LIMITATIONS
The major limitation of this study is the small sample size. However by ensuring use of consistent methodology, combining two cohorts for a larger sample was possible. Further research with larger groups of both graduate-entry and undergraduate nursing students is required, as these results require follow-up. Replication of the teaching is possible; however student placements will differ across programmes, therefore this aspect of the research is not possible to replicate.
CONCLUSION
Nursing students, like qualified nurses and other health-care professionals, are not shielded from experiencing aggression and violence during clinical placements, an issue exacerbated by the COVID-19 pandemic. While the educational intervention “It’s all about communication” resulted in increases in nursing students’ confidence in dealing with aggressive patients and enhanced their competence in interpersonal communication, further research into the long-term outcomes of this educational intervention would be helpful. This could focus on student attrition rates, choice of area of work and transference of learned communication skills to clinical work, post-registration. The improvement in confidence and communication from baseline to acute care is greater than that from acute care to mental health, indicating that delivering the intervention earlier in the nursing programme rather than before the mental health placement was useful for nursing students. It meant they could look broadly at communication skills and dealing with aggression or a crisis as not only being part of mental health nursing but as applicable across all areas of their work. This study highlights the need to deliver communication skills training early in nursing education to enable nursing students to develop confidence in dealing with aggression across all areas of health care.
Footnote
1) In July 2022, New Zealand’s 20 district health boards, which delivered or funded all public health services, were replaced by a single body, Te Whatu Ora – Health New Zealand.
REFERENCES
Ang, W. C., Swain, N., & Gale, C. (2013). Evaluating communication in healthcare: Systematic review and analysis of suitable communication scales. Journal Of Communication In Healthcare, 6(4), 216-222.
Baby, M., Gale, C., & Swain, N. (2018). A communication skills intervention to minimise patient perpetrated aggression for healthcare support workers in New Zealand: a cluster randomised controlled trial. Health & Social Care in the Community, 27(1), 170-181.
Bilgin, H., Ozcan, N. K., Tulek, Z., Kaya, F., Boyacioglu, N. E., Erol, O., Coban, S. A., Pazvantoglu, O., & Gumus, K. (2016). Student nurses’ perceptions of aggression: An exploratory study of defensive styles, aggression experiences, and demographic factors. Nursing and Health Sciences, 18, 216-222.
Brann, M., & Hartley, D. (2017). Nursing student evaluation of NIOSH workplace violence prevention for nurses’ online course. Journal of Safety Research, 60, 85-91.
Duxbury, J., & Whittington, R. (2005). Causes and management of patient aggression and violence: staff and patient perspectives. Journal of Advanced Nursing, 50(5), 469-478.
Dyer, O. (2021). US hospitals tighten security as violence against staff surges during pandemic. BMJ, 375, n2442.
Franz. S., Zeh, A., Schablon, A., Kuhnert, S., & Niehans, A. (2010). Aggression and violence against healthcare workers in Germany – A cross-sectional retrospective survey. BMC Health Services Research, 10, 51.
Guay, S., Goncalves, J., & Boyer, R. (2016). Evaluation of an Education and Training Program to Prevent and Manage Patients’ Violence in a Mental Health Setting: A Pretest-Posttest Intervention Study. Healthcare, 4, 49.
Hahn, S., Hantikainen, V., Needham, I., Kok, G., Dassen, T., & Halfens, R. J. G. (2012). Patient and visitor violence in the general hospital, occurrence, staff interventions and consequences: a cross-sectional survey. Journal of Advanced Nursing, 68(12), 2685-2699.
Hallet, N., Wagstaff, C., & Barlow, T. (2021). Nursing students’ experiences of violence and aggression: A mixed-methods study. Nurse Education Today, 105, 1-6.
Heckemann, B., Zeller, A., Hahn, S., Dassen, T., Schols, J. M. G. A., & Halfens, R. J. G. (2015). The effect of aggression management training programmes for nursing staff and students working in an acute hospital setting. A narrative review of current literature. Nurse Education Today, 35, 212–219.
Hopkins, M., Fetherston, C. M., & Morrison, P. (2014). Prevalence and characteristics of aggression and violence experienced by Western Australian nursing students during clinical practice. Contemporary Nurse, 49(1), 113-121.
International Labour Office (ILO), International Council of Nurses (ICN), World Health Organization (WHO), & Public Services International (PSI). (2002). Joint programme on workplace violence in the health sector. ILO.
Jackson, D., Hutchinson, M., Everett, B., Mannix, J., Peters, K., Weaver, R., & Salamonson, Y. (2011). Struggling for legitimacy: nursing students’ stories of organisational aggression, resilience and resistance. Nursing Inquiry, 18(2), 102-110.
Jeong, Y. & Lee, K. (2020). The development and effectiveness of a clinical training violence prevention program for nursing students. International Journal of Environmental Research and Public Health, 17, 4004.
Magnavita. N., & Heponiemi, T. (2011). Workplace violence against nursing students and nurses: An Italian experience. Journal of Nursing Scholarship 43, 203–210.
Minton, C., Birks, M., Cant, R., & Budden, L. M. (2018). New Zealand nursing students’ experience of bullying/harassment while on clinical placement: A cross-sectional survey. Collegian, 25(6), 583-589.
National Institute of Occupational Safety and Health (NIOSH). (2021). Occupational Violence.
Nau, J., Dassen, T., Needham, I., & Halfens, R. (2009). The development and testing of a training course in aggression for nursing students: a pre-and post‐test study. Nurse Education Today, 29(2), 196‐207.
Nau, J., Dassen, T., Needham, I., & Halfens, R. (2011). Sensitivity, specificity and predictive value of Confidence in Managing Patient Aggression Scale on de-escalating behaviour. Journal of Clinical Nursing, 20, 2584–2586.
Nowrouzi-Kia, B., Isidro, R., Chai, E., Usuba, K., & Chen, A. (2019). Antecedent factors in different types of workplace violence against nurses: a systematic review. Aggression and violent behavior, 44, 1-7.
Occupational Safety and Health Administration (OSHA). (2016). Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers. U.S. Department of Labor.
Ross, L., Boyle, M., Williams, B., Fielder, C., & Veenstra, R. (2014). Perceptions of student paramedic interpersonal communication competence: A cross-sectional study. Australasian Journal of Paramedicine, 11(4).
Rubin, R. B., & Martin, M. M. (1994). Development of a measure of interpersonal communication competence. Communication Research Reports, 11(1), 33-44.
Shafran-Tikva, S., Chinitz, D., Stern, Z., & Feder-Bubis, P. (2017). Violence against physicians and nurses in a hospital: How does it happen? A mixed-methods study. Israel Journal of Health Policy Research, 6, 59.
Silverman, J., Kurtz, S., & Draper, J. (2013). Skills for communicating with patients (3rd ed.). Radcliffe.
Story, A. R., Harris, R., Scott, S. D., & Vogelsmeier, A. (2020). An evaluation of nurses’ perception and confidence after implementing a workplace aggression and violence prevention training program. Journal of Nursing Administration, 50(4), 209-215.
Swain, N., Gale, C., & Greenwood, R. (2014). Patient aggression experienced by staff in a public hospital setting. New Zealand Medical Journal, 127, 1394.
Swain, N., & Gale, C. (2014). A communication skills intervention for community healthcare workers: Perceived patient aggression is reduced. International Journal of Nursing Studies, 51(9), 1241-1245.
Te Pou. (2016). Safe Practice Effective Communication.
Thackrey, M. (1987). Clinician confidence in coping with patient aggression: Assessment and enhancement. Professional Psychology: Research and Practice, 18(1), 57-60.
Warshawski, S. (2021). Workplace violence directed at nursing and medical students – What can students tell us about it? Journal of Professional Nursing, 37(6), 1110-1118.
Winstanley, S., & Whittington, R. (2004). Aggression towards healthcare staff in a UK general hospital: Variation among professions and departments. Journal of Clinical Nursing, 13(1), 3-10.
WorkSafe New Zealand. (2016). WorkSafe’s Strategic Plan for Work-Related Health 2016 to 2026.
Daily doses – uncut news
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


