About the authors:Ruth McChesney, RN, BHSc(hons)nsg, PGDipHlthSci, NZCertBus(first line management), is an acute demand specialist nurse at the Western Bay of Plenty Primary Health Organisation, Tauranga, New Zealand. Patricia McClunie-Trust, RN, PhD, is a principal academic staff member in the Centre for Health and Social Practice, Waikato Institute of Technology, Hamilton, New Zealand. This article was accepted for publication in October 2021. |
ABSTRACTBackground: Access to community palliative and end-of-life care that is patient-centred, culturally sensitive and responsive is not equitable for all people in New Zealand. There is an opportunity to transform primary palliative care through an anticipatory prescribing approach and an interdisciplinary workforce. Research is needed to inform the development of best practice and give confidence to authorised prescribers. Aim: This study aimed to identify the factors influencing anticipatory prescribing in community palliative and end-of-life care. Methodology: A literature search was undertaken of the databases CINAHL Complete, Science Direct, PubMed, Google Scholar, Grey Lit, Open Grey, Mednar and Open Core. Seven relevant primary research studies were selected. A meta-synthesis of the qualitative research was carried out using a critical realist framework. Findings: Three main themes emerged from the reviewed articles to explain the factors influencing anticipatory prescribing in community palliative and end-of-life care, including expertise, teamwork and prioritisation. Expertise had two subthemes, which were knowing when to prescribe and knowing how to prescribe. Conclusions: Developing and maintaining expertise in primary palliative care, developing better interdisciplinary teamwork, and the prioritising of this prescribing practice are the factors underpinning effective anticipatory prescribing in palliative and end-of-life care. There is an ethical responsibility to anticipate the likely deterioration and end-of-life needs of palliative patients, so timely care can be provided and symptoms managed. Anticipatory prescribing should be individualised, approached with an equity lens, and delivered through an interdisciplinary health workforce to effectively meet population needs. |
||
KEYWORDSpalliative, end-of-life care, anticipatory prescribing, patient/whānau-centred, interdisciplinary team, community |
|||


INTRODUCTION
INTERDISCIPLINARY TEAMWORK IS INTEGRAL to the philosophy of palliative care (Brown, 2015). The complexities of whole-person care require the complementary approaches of different team members to work together to meet the needs of the patient and their whānau or family (Dyess et al, 2020; Ministry of Health [MoH], 2012). Relieving physical suffering is an important component of palliative and end-of-life care, an intervention which should not have to be delayed (Rome et al, 2011). Predicting when patients’ end-of-life will occur remains a significant challenge to health professionals, however, and responding to acute needs at short notice can present a challenge to general practices in New Zealand.
The approach of anticipatory prescribing for palliative and end-of-life care needs is used overseas (Antunes et al, 2020; Brady, 2016) and has the potential to provide timely and more equitable access to symptom control here in New Zealand. This article reports on a meta-synthesis of qualitative research, applying a realist framework to better understand the factors affecting anticipatory prescribing in community palliative and end-of-life care.
BACKGROUND
Anticipatory prescribing is the approach of prescribing medications ahead of clinical need for symptoms that are likely to occur, so the medications are readily available when they are needed most (National Clinical Guideline Centre, 2015). Anticipatory prescribing is used for end-of-life care to reduce potential distress or suffering. This approach can also be used in the management of long-term and palliative-stage conditions, where providing medication in advance of likely recurrent symptoms can enable treatment to be initiated sooner before a worsening deterioration develops. Meeting people’s palliative and end-of-life care needs is internationally recognised as a basic human right (World Health Organization, 2020). The burden of disease and the changes that take place when dying mean that there is potential for suffering, which can often be avoided.
Palliative care aims to improve an individual’s quality of life until their death, attending to their physical, psychosocial and spiritual needs in a culturally sensitive way (MoH, 2011). For care to be fairly distributed, patients should have equitable access to care. However, in New Zealand, significant health disparities are known to exist between Māori and non-Māori, including in accessing palliative care (MoH, 2014). Māori have a higher incidence of life-limiting disease, yet their access to palliative care has failed to match their need (Kidd et al, 2018). Despite the principles and obligations under Te Tiriti o Waitangi (The Treaty of Waitangi), to preserve and improve health for Māori, equitable provision of palliative care has not been achieved in New Zealand (MoH, 2019). There are also other inequities in palliative care that are not specific to Māori, relating to non-cancer diagnoses, age, other minority ethnicities, and rural geographical locations, which need to be addressed for care to be fairly distributed (Palliative Care Council of New Zealand, 2010).
The palliative death rate in New Zealand is projected to increase by more than 47 percent over a 22-year period, from 30,500 deaths in 2016 to 45,000 deaths in 2038 (McLeod, 2016; see Table 1, below).
Table 1: Projected palliative deaths in New Zealand
| Year | Number of deaths | Change |
|---|---|---|
| 2016 | 30,500 | 47.5% (over 22 years) |
| 2038 | 45,000 |
The three most common categories of palliative deaths relate to the circulatory system, cancer, and “other” causes, which largely encompasses dementia and frailty (McLeod, 2016; see Table 2, below).
Table 2: Most common causes of palliative deaths
| Year | 1 (most common) | 2 | 3 |
|---|---|---|---|
| 2016 | circulatory system | cancer | other (includes dementia, frailty) |
| 2038 | circulatory system | other | cancer |
By 2038, non-cancer related deaths are expected to reach triple the number of cancer deaths (McLeod, 2016).
As cancer has a more predictable disease trajectory than other palliative diseases, the projected increase in non-cancer related deaths will result in less predictable patterns of illness, including the onset of patients’ last days of life (Thomas et al, 2016). Over the coming decades, death rates for Māori are expected to stay constant, but those deaths are projected to occur at much older ages (McLeod, 2016). Considering Māori are currently under-represented in the uptake of palliative care (Kidd et al, 2018), achieving equity will involve matching the current need and increasing resources to match the rising need (MoH, 2016).
International studies indicate that most people prefer to die at home (Grattan Institute, 2014; Nilsson et al, 2017; Pennec et al, 2015; Stanford School of Medicine, 2021). However, in New Zealand, over a third of adults aged 65 and over die in acute hospitals (Broad et al, 2015). Data on place of death suggests that there is poor continuity of care and support being provided at home (MoH, 2016) which can lead to crises (which may involve suffering and harm) and care being provided contrary to the patient’s wishes. Furthermore, there are quality and sustainability concerns, which may result in poorer outcomes for patients and families (Health Quality & Safety Commission [HQSC], 2020). These concerns are likely to compound, resulting in significantly strained resources for future palliative patients if not addressed (HQSC, 2020).
Enabling anticipatory prescribing to become a safe and widespread practice would require a true integration of services. For example, anticipatory care plans and prescriptions could primarily be developed by GPs and primary care nurse practitioners (NPs). They could also be initiated by secondary and specialist care providers, with a request for review by the patient’s primary provider within a defined timeframe. As outlined in the Resource and Capability Framework for Integrated Adult Palliative Care Services (MoH, 2012), most palliative care would continue to be provided by primary care providers, with support from specialist services. However, the anticipatory care plans and prescriptions could be accessed by other community health-care providers as appropriate, allowing them to provide care whenever needed, according to the patient’s wishes and the directives of the primary provider.
METHODOLOGY
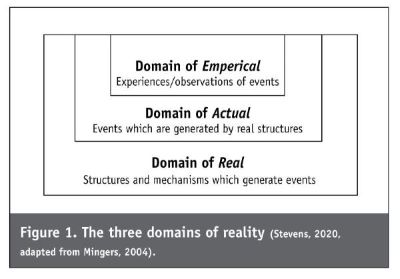
The origins of critical realism come from the writings of Roy Bhaskar, who made the distinction between epistemology, a focus on knowledge, and ontology, a focus on reality (Archer et al, 2013; Bhasker, 1975). The underpinning philosophy of realism deals with the truths behind what is unobservable, seeking to understand the causal processes between the context of an intervention and the outcomes (Chakravartty, 2017). Informed by the three domains of reality (see Figure 1, below), theory or data can be evaluated through four basic forms of logic: deductive, inductive, abductive and metaphoric inference (Eastwood et al, 2014). Retroduction can then be used to conceptualise the hidden causal forces that emerge from these forms of logic. The result (see Figure 1) is a layered approach to explaining the mechanisms that result in particular outcomes within particular contexts.
Applying a realist review approach to a synthesis of the findings of primary research studies can enable a deeper understanding of these causal processes.
Realist review approach
The methodological process followed in this review was informed by the realist review stages outlined by Power et al (2019). According to Power et al, there are six active stages in carrying out a realist review.
- Stage 1: Setting a clear scope for the review and developing a theoretical framework.
- Stage 2: Creating a search strategy.
- Stage 3: Selecting and appraising the primary research studies.
- Stage 4: Undertaking a process of data extraction.
- Stage 5: Data synthesis and analysis processes.
- Stage 6: Testing and refining theories that have been developed.
These six stages were adapted to form a basis for the methodology for this study. Elements of the PICO (population, intervention, context and outcome) were identified as authorised prescriber, anticipatory prescribing, community palliative and end-of-life patients, and symptom management respectively, as represented in Table 3 below.
Table 3: PICO table
| Key words | Synonyms and other terms | |
|---|---|---|
| Population | Authorised prescriber | General practitioner, GP, nurse practitioner, NP, nurse prescriber, family doctor, family physician. |
| Intervention | Anticipatory prescribing | Advanced prescribing, pre-emptive prescribing, just-in-case medications. |
| Context | Community palliative and EOL patients | Palliative, last days of life, terminal, dying. Home, primary care, community. |
| Outcome | Symptom management | Symptom relief, “good death” vs “bad death”. |
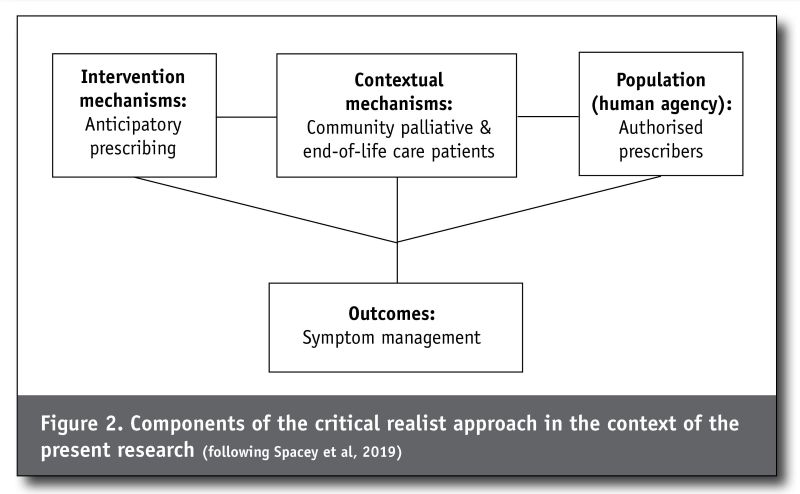
To apply these elements of the PICO to a critical realist framework, the intervention and context were considered as mechanisms, the population viewed as human agency, and the outcome was viewed as an inter-relation of the above, as shown in Figure 2 below.
Search strategy:The second stage involved refining and completing the search strategy. The terms from the PICO table were used as a basis for searching databases. The terminology used in other countries was explored to maximise the capture of international findings. The search strategy for PubMed is shown in Box 1, and was adapted for CINAHL Complete, Science Direct, Google Scholar, Grey Lit, Open Grey, Mednar and Open Core.
Box 1: PubMed search strategy
“symptom control” OR “symptom management” OR “symptom relie*” OR “suffering” OR “distress” AND “palliative” OR “end stage” OR “terminal” OR “last days of life” AND
“anticipatory prescribing” OR “anticipatory medication” OR “just in case prescribing” OR “just in case medication” OR “end-of-life prescribing” OR “end-of-life symptom
management” OR “end-of life medication” AND “authorised prescriber” OR “authorized prescriber” OR “medical
practitioner” OR “general prescriber” OR “GP” OR “nurse
practitioner” OR “NP” OR “prescriber” OR “family doctor” OR “family physician”
FILTERS: in the last 10 years
LIMITS: publication year ≥2011, research article/
primary research
EXCLUDES: guidelines, quantitative, secondary research
Study selection: Inclusion and exclusion criteria were applied to the selection of studies. Primary research studies published in the last 10 years were included. Anticipatory prescribing in contexts other than palliative and end-of-life care were excluded. Articles not published in English were excluded unless an English translation was available. Additional relevant articles were handpicked from the reference lists of secondary research studies to add completeness and rigour. The PRISMA process diagram (Figure 3) shows the identification of the studies selected at each stage.
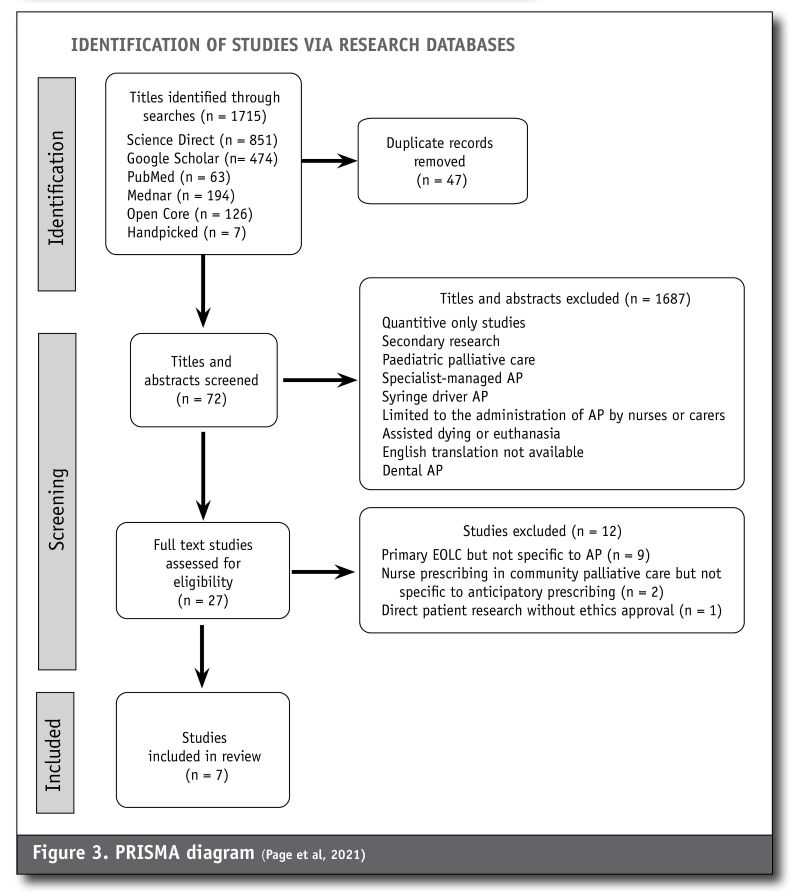
Data extraction: Research article titles were screened to indicate whether the topic was potentially relevant, and if so, the abstract was screened. Article titles which included palliative, terminal, dying, last days of life, or symptom management, had their abstracts screened. If articles were found to be exclusive to hospital anticipatory prescribing, prescribing for assisted dying, or involved examining decisions about the administration of anticipatory medications for example, they were excluded. During the full-text review, 11 of the articles were found ineligible on the basis of not directly mentioning anticipatory prescribing.
Quality appraisal: The Joanna Briggs Institute (JBI, 2017) critical appraisal checklist was used as assessment criteria for all seven articles. Three of the 10 appraisal areas highlighted some areas which were lacking strength. Three studies did not locate the researcher culturally or theoretically. Two studies did not address the influence of the researcher and there was a level of uncertainty with two further studies of this being adequately addressed. The final area of potential inadequacy was in two studies which did not provide reader assurance that the voices of the study participants were adequately represented. One article was excluded since it did not demonstrate ethical review in a study involving palliative patients as the population.
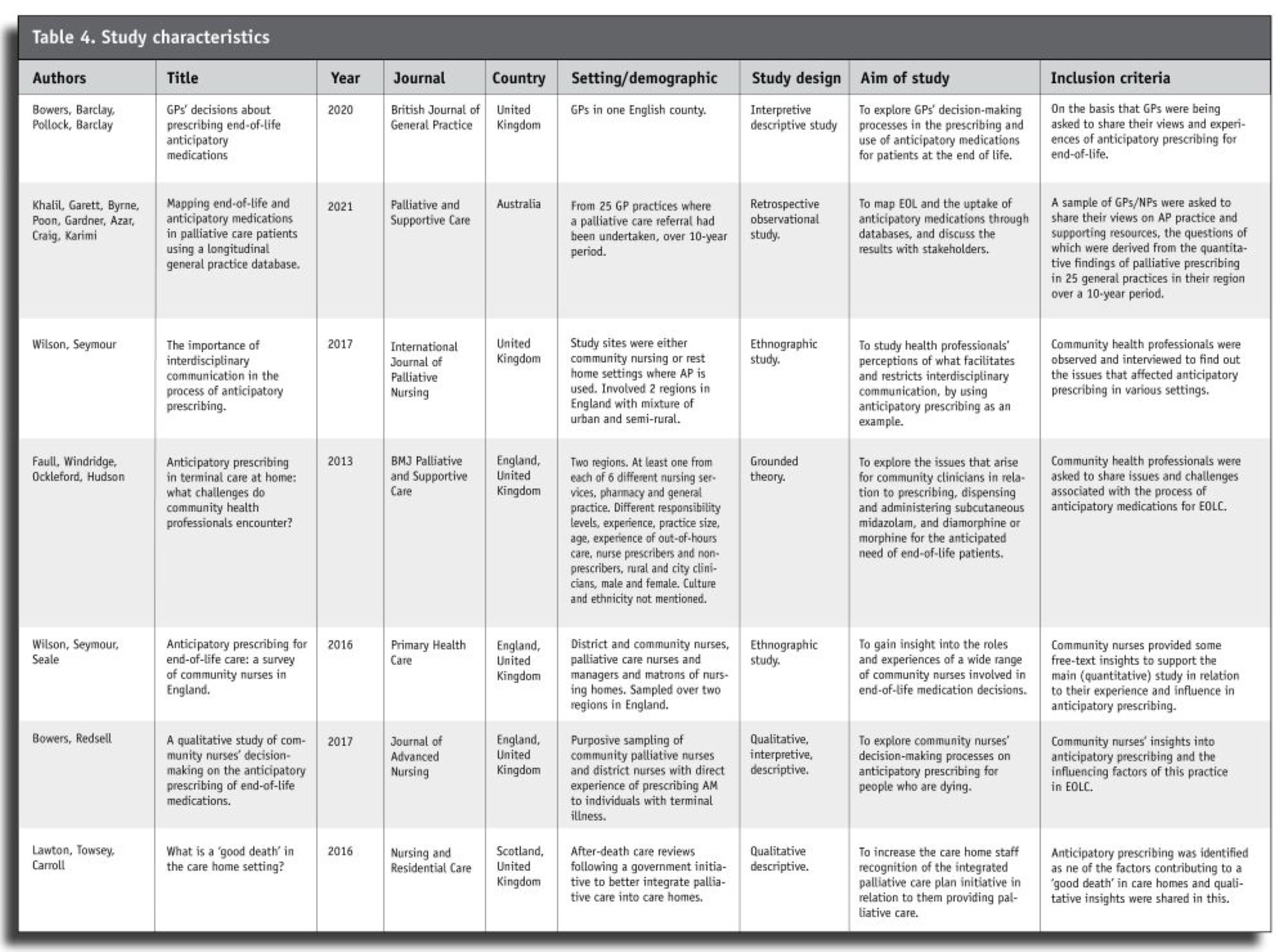
Characteristics of the selected studies: The characteristics of the seven studies selected for inclusion in the review are set out in Table 4 (below). Five of the studies were English, one was Scottish (of note: the National Health System (NHS) in England and Scotland are separate health system bodies). The seventh study took place in Victoria, Australia (Khalil et al, 2021). The community settings had GP or nurse practitioner clinical oversight, with interdisciplinary team involvement. Aged residential care homes were included as a community setting; hospice in-patient units were excluded.
The seven studies were published between 2012 and 2021 in general practice, nursing and palliative care journals. Three study designs were qualitative descriptive, two were ethnographic, one was observational and one was based on grounded theory. Although Bowers et al (2020) note that anticipatory prescribing is encouraged practice for end-of-life symptom management in the United Kingdom (UK), Australia and New Zealand, no New Zealand-based studies were located.
Data synthesis & analysis: The Stepwise Framework (Bygstad et al, 2016) was used to guide the stages of data analysis and synthesis. This framework was chosen for the six-step process it provides with an applied critical realist approach (Table 5).
Table 5
| Data synthesis and analysis |
|---|
| 1. Description of events and issues that constitute the phenomenon of interest. |
| 2. Identification of key entities. |
| 3. Theoretical re-description (abduction). |
| 4. Retroduction
a) immediate outcomes |
| 5. Analysis of the set of affordances and associated mechanisms. |
| 6. Assessment of explanatory power. |
The first step involved noting the events and issues that lead to anticipatory prescribing from each of the seven studies. The second step involved identifying the key entities that constituted structures with causal powers (Bygstad et al, 2016). By the third step, an exploration of meaning was applied, where through abduction, themes to explain and interpret the events were noted. The fourth step, made up of four sub-steps, involved going through the data with retroductive inference, a process of identifying the circumstances where anticipatory prescribing would not occur. The analysis as part of step five involved explaining the causal properties of the events and how they related to dependent factors and contributed to mechanisms. Finally, in step six, the explanations of the causal properties and mechanisms were tested repeatedly against the theorising already made, and the wording of these was refined until the explanatory power was most effectively explained (Power et al, 2019). Once the explanations had been tested, the coding of data was compiled in a table under the explanatory themes.
FINDINGS
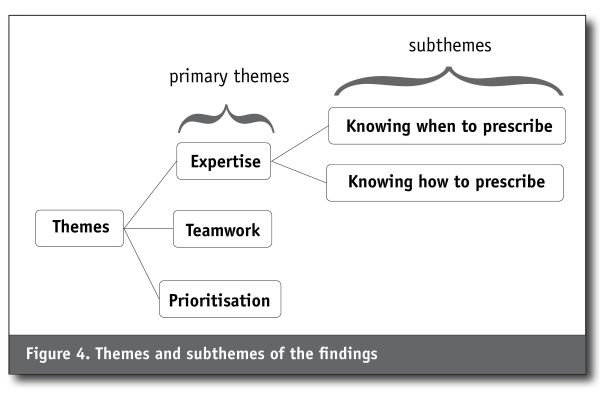
Three primary themes emerged from the synthesis, including expertise, teamwork and prioritisation. Expertise has two subthemes, which are knowing when to prescribe, and knowing how to prescribe (see Figure 4).
Expertise
Effective anticipatory prescribing for palliative and end-of-life care needs is underpinned by expertise. This idea of expertise is reflected in the primary research findings referring to “getting the timing right” (Bowers et al, 2020); “knowledge of when to prescribe” (Khalil et al, 2021); “awareness of pathways” (Khalil et al, 2021); “knowledge of publicly available resources” (Khalil et al, 2021); “reflecting on expertise and experience” (Faull et al, 2013); and in “reading the situation” (Bowers & Redsell, 2017). A well-placed confidence to prescribe for palliative and end-of-life care comes from knowledge and experience (Wilson et al., 2016) and through education, such as from local integrated projects for palliative care which include guidance on anticipatory prescribing (Lawton et al, 2016). Knowing “when” and knowing “how” to prescribe anticipatory medications both require expertise.
Knowing when to prescribe: Knowing when to prescribe anticipatory medications requires the greatest expertise. It is challenging to accurately predict when symptoms will occur, and identifying the right stage to prescribe anticipatory medications is also a challenge and significant barrier to its implementation (Bowers & Redsell, 2017; Khalil et al, 2021). Some prescribers only use anticipatory prescribing for end-of-life. Others prescribe for earlier stages, aware that there are additional benefits and indications for anticipatory prescribing (Khalil et al, 2021). Noticing that a patient is deteriorating is the most obvious indication for which prescribers agree to prescribing anticipatory medications; there will likely be a consensus too, if the practitioner can anticipate the patient’s disease deterioration (Khalil et al, 2021). Nurses also make judgements about when anticipatory prescribing may be appropriate, initiating conversations with families and recommending that GPs consider anticipatory prescribing (Bowers & Redsell, 2017; Wilson et al, 2016). These clinical judgements by the nurse may or may not be shared by the prescriber (Wilson et al, 2016). Some GPs, on the other hand, fully rely on nurses to prompt them to consider anticipatory prescribing, particularly in aged residential care (Bowers et al, 2020).
Knowing when to prescribe is a learnt skill (Bowers & Redsell, 2017; Faull et al, 2012). Prescribers need a forward-planning approach and may tie in the timing of anticipatory prescribing with other care-planning decisions such as resuscitation status and preferred place of care and death (Bowers et al, 2020). Interdisciplinary team meetings provide shared expertise and lead to shared decision-making on when to prescribe anticipatory medications (Wilson & Seymour, 2017). The Gold Standards Framework (GSF), a tool designed to help clinicians develop a more planned approach to life-limiting conditions (Thomas & Noble, 2007), forms the basis and purpose of interdisciplinary team meetings (Wilson & Seymour, 2017).
“In our practice, we have regular Gold Standard Framework meetings where we keep up to date on what’s happening with the patients. The district nurses normally let me know when anticipatory drugs are needed.”
(GP interview, Wilson & Seymour, 2017, p 131).
This quote provides an example of where patient care is improved by different professions working together. The different lens they bring from their clinical backgrounds, experience and working contexts adds more than an individual practitioner or single-disciplinary team are likely to provide.
Knowing how to prescribe: The skill in knowing how to prescribe has several important elements. Best practice in prescribing dictates that prescribers must know the patient’s condition well, have undertaken adequate assessment of the patient’s situation, and know that the medications are safe and appropriate for the patient’s needs (General Medical Council, 2021; Medical Council of New Zealand, 2020). Most GPs report seeing the patient for themselves following a nurse suggesting anticipatory prescribing, but a minority would prescribe on account of a well-known and trusted nurse (Bowers et al, 2020). Conversations with patients and their families about anticipatory prescribing need skill and sensitivity, tailored at a level that matches their needs (Bowers et al, 2020). Although some patients and families are open to talking about the need for anticipatory prescribing and are believed to be reassured by it being implemented, others have appeared ambivalent. GPs report framing anticipatory prescribing as a clinical recommendation, while giving the patient and family the opportunity to opt out (Bowers et al, 2020). GPs need to know where to find appropriate guidance, otherwise they may be unlikely to prescribe anticipatory medications (Wilson & Seymour, 2017).
A final but significant element of knowing how to prescribe is in the correct completion of prescriptions. Wilson et al’s (2016) study of 575 community nurses involved with palliative care revealed that incorrectly prescribed anticipatory medications affected around one fifth of nurses. GPs seemed to lack understanding of the impact of incomplete prescriptions on their interdisciplinary colleagues. What GPs considered small errors in their prescriptions, were in fact legally incomplete prescriptions/documents for pharmacists to dispense or nurses to administer. However, the lack of understanding about these differing responsibilities led to time-consuming processes, delays in access to medications and considerable frustration on both sides. Skill and experience could lead to more accurate prescriptions being written, and improved understanding of professional colleagues’ responsibilities.
“If we get a form right, it’s usually cause for celebration. Just because all of the ‘I’s and all of the ‘T’s definitely have to be crossed. I’m not sure they actually definitely have to be crossed but our district nurses feel that they actually have to definitely be crossed”.
(GP interview, Wilson & Seymour, 2017, p 132)
“I think sometimes doctors don’t seem to understand the importance, the legal requirements of doing a controlled drug prescription. For example, the validity, there’s got to be directions, dosage, quantity, they’ve got to be in words and figures . . . There’s times when prescriptions come from surgeries that haven’t been signed, where legally you cannot dispense it then”.
(Pharmacist interview, Wilson & Seymour, 2017, p 132).
Inexperience – the opposite to expertise – leads to a reluctance to do anticipatory prescribing and results in variations in practice between prescribers (Faull et al, 2013; Wilson & Seymour, 2017; Wilson et al, 2016). The fears documented about anticipatory prescribing include prescribing opioids, expediating death, misuse, waste, and medication shortages, which lead to reluctance and in turn, less real-world experience of using this approach (Bowers & Redsell, 2017; Faull et al, 2013; Khalil et al, 2021). For more experienced clinicians, misuse and waste are viewed as risks rather than fears, and risks are weighed up against the potential benefits. While there may be risks involved in putting medications in a house too early, the possibility that individuals may not get effective symptom management if left too late is often a greater cause for concern (Bowers & Redsell, 2017). In cases where medications were left in homes for longer periods, experienced GPs would rely on nurses to provide feedback on any concerns they had (Bowers et al, 2020).
Teamwork
The process of anticipatory prescribing is smoother and more successful when health professionals work as a team. Nurses were often the first to identify the need for anticipatory prescribing (Wilson & Seymour, 2017) and GPs typically assumed responsibility for initiating the anticipatory prescribing conversations with the family (Bowers et al, 2020). Nurse prescribers would often take responsibility for both. They initiated conversations both with the family unit and the GP, having the authority to prescribe independently within their scope, but with the aim to act collaboratively (Stenner & Courtenay, 2008).
GPs were reported as being receptive to nurses requesting that they consider anticipatory prescribing, were influenced by them, valued them greatly, and frequently relied on them (Bowers et al, 2020). Specialist and palliative care nurses were considered an asset to GPs, and nurses were aware that they were acting as the eyes and ears of the GPs (Bowers & Redsell, 2017; Bowers et al, 2020; Wilson & Seymour, 2017). However, as non-specialised providers of palliative care, district nurses could feel undervalued and not listened to by GPs, in many cases stemming from hierarchical attitudes and poor understandings of nurses’ responsibilities and capabilities (Wilson & Seymour, 2017). Other studies contrasted with this finding, showing that district nurses formed closer relationships with GPs than specialist nurses (Bowers & Redsell, 2017). The reason for this was that GPs and specialist nurses could both attempt to take the lead, and as a result experience conflict. Specialist nurses were also thought to value specialist palliative views over the generalist views of GPs (Bowers & Redsell, 2017).
In all cases, an adequate nurse-GP (or other prescriber) relationship needs to be established (Bowers & Redsell, 2017). An understanding of differing professional responsibilities is also vital. When these aspects of connection and relationship are properly understood, it can lead to increased communication and trust in the anticipatory prescribing process. In contrast, lack of trust and/or relationship tends to be the weak link in the process of anticipatory medications in the home (Faull et al, 2013).
“I offered to meet the out-of-hours doctor, it was a . . . patient who was very, very terminally ill and he said he would, but didn’t, and he . . . admitted that patient and she died in the ambulance on the way to hospital and you know, that was – I was quite happy to meet him, to give whatever, but he wasn’t interested.”
(Nursing professional, focus group 8, Faull et al, 2013, p 3).
“We had a patient who was requiring an awful lot of morphine . . . the breakthrough dosages were very high and were continually being adjusted and because [specialist palliative nurses] were involved I used to give quite a big range actually, because they were women that I worked with . . . and I know and trust, so you give a big range . . . but when you have a [different] nurse going in at night, they were very, very reluctant to give the dose that they had been having and they would tend to go to the lowest dose on the range, which caused difficulty with pain control . . . not knowing the patient, not knowing the family, not knowing me, not knowing the team, and being asked to give what seemed to be a lethal dose of morphine.”
(GP interview 2, Faull et al, 2013, p 4).
The health professionals in these examples appear to have acted independently, rather than as part of a team, highlighting that insufficient links between them prevent a more comprehensive approach to care. Nurses working in aged residential care, in relative isolation from the health-care team, may request admission of palliative patients to hospital, which may later be identified as inappropriate (Lawton et al, 2016). Having one GP allocated to an aged care home has the potential to improve the relationship and trust between members of the health team in this context (Wilson & Seymour, 2017), as it promotes continuity of relationship as well as continuity of care. Nurses advocating for patients in aged care settings have successfully promoted collective discussions about anticipatory medications (Bowers et al, 2020).
Where nurses work well with GPs, they report good access to anticipatory medications (Faull et al, 2013). Being located in the same building enhances relationships; the closer the proximity, the more frequently the informal “corridor” conversations take place (Wilson & Seymour, 2017). When nurses have been overstretched in their workload or split off from GPs geographically, it has made their working relationships, interdisciplinary communication, and the process of anticipatory prescribing more difficult (Bowers et al, 2020). One solution has been having the GP review the shared electronic records where nursing care is documented. Anticipatory prescribing was also reportedly used as a signal to visiting clinicians that symptom control was the priority focus when shared electronic records were not available (Bowers et al, 2020).
Nurses know to provide regular updates to GPs in relation to patients who may need anticipatory medications (Bowers & Redsell, 2017). Yet nurses encounter issues with some GPs when they broach the subject of anticipatory prescribing. Even senior nurses with direct experience in anticipatory prescribing reported “playing the game” when negotiating with GPs over what to prescribe. Nurses are documented as having to balance the patient advocacy role with negotiation tactics – compromises, persuasions, suggestions and tailored approaches to individual GPs (Bowers & Redsell, 2017). However, healthy negotiations tend to be valued by nurses, like in the following example.
“It’s very rare that your suggestions are ignored. The problem is I don’t like the doctors that say no to everything and I don’t like doctors who say yes to everything, I like the negotiation.”
(Rene, community palliative nurse, Bowers & Redsell, 2017, p 18).
Even when conflicts arise, nurses would work to get the best outcome for the patient.
“They don’t always agree with me and sometimes you have to choose your battles, but ultimately you have got to do what’s right for the patient . . . I’m not afraid to be the advocate and push that forward.”
(Debbie, community palliative nurse, Bowers & Redsell, 2017, p18).
GPs also put their patients’ needs above that of concerns within the interdisciplinary team. For example, concern would arise if the GP had no connection with the third party who would be initiating the anticipatory medications. However, the greater concern for GPs was that the patient would not be given the prescribed medication when needed, and that this would result in a bad death (Bowers et al, 2020). Ultimately, health professionals are still navigating interprofessional issues to continue to provide the safest and most effective patient care they can.
Prioritisation
Recognising the benefits of anticipatory prescribing, and acting to prioritise them, is the third theme to emerge from the analysis. The prescribers involved in facilitating anticipatory prescribing were aware of the benefits it could bring to patients and their families; to relieve distressing symptoms when they occurred meant caring for the physical needs of the patient, and offering a sense of control to patients and their families in knowing that these needs could be managed (Bowers & Redsell, 2017).
“I like to have those conversations early. To get them out of the way sounds like I’m trying to avoid them, I think get them out of the way for their benefit so that they don’t have to, they can, there’s a lot to sort out, ‘let’s get it all sorted out and then enjoy the last time you have’.”
(Dr Matthews, GP and out-of-hours doctor, Bowers et al, 2020, e734).
Anticipatory prescribing was seen as an insurance plan, a way of managing uncertainty and preventing crises, particularly for non-cancer conditions where disease trajectories could be very difficult to predict (Bowers et al, 2020). In these patients, anticipatory prescribing was done while the patient was still stable, and could involve medications to cover end-of-life symptoms as well as earlier needs (Bowers et al, 2020; Khalil et al, 2021). Only some clinicians used anticipatory medications to manage other stages of late disease and specifically injectable medications in patients for whom oral medications were no longer best, for example, when swallowing issues were present and gastroparesis (Bowers et al, 2020; Khalil et al, 2021). Having a proactive mindset enabled GPs to put anticipatory medications in place before the clinical needs occurred. Knowing the benefits of anticipatory prescribing is the first step in this; prioritising the action is the next, even if the need does not arise for a while.
“One or two of the partners said, ‘I think it’s a problem thinking when to do it’. I said, ‘Why? Why can’t you just leave it [anticipatory medications] gathering dust . . . why can’t you do it early?’ ”
(Dr Taylor, GP, Bowers et al, 2020, p3)
While some GPs felt it was the responsibility of out-of-hours services to attend to end-of-life symptomatic needs (Wilson et al, 2016), many other GPs felt anticipatory prescribing was a more optimal approach to covering out-of-hours care needs (Bowers et al, 2020; Bowers & Redsell, 2017). Anticipatory prescribing was therefore put in place to benefit patients and their families, as well as to prevent additional work for their out-of-hours colleagues (Bowers et al, 2020). The risks of leaving medications in homes for months where they could go missing, be misused or expire are well documented, and in some contexts accessing these medications to begin with could be challenging, and the cost could affect patients (Bowers et al, 2020; Faull et al, 2013; Khalil et al, 2021). However, for many GPs these challenges were worked around, whenever the clinical and emotional benefits outweighed the risks (Bowers et al, 2020).
As a result of the anticipatory prescribing approach, many GPs found working in palliative care extremely rewarding, and were willing to work hard to prioritise end-of-life symptom control (Bowers et al, 2020). This willingness cultivated a culture where anticipatory prescribing was encouraged (Bowers et al, 2020). Ultimately there was also agreement on the principle that distressed patients should not have to wait for relief, that without anticipatory prescribing “bad deaths” occurred, and “good deaths” could occur where anticipatory prescribing was present (Faull et al, 2013; Lawton et al, 2016).
“Just in case [JIC] drugs used 3 times in the last 24 hours of life – family delighted with the care.”
(Afterdeath review in Care Home, number 12, Lawton et al, 2016, p 496).
Anticipatory prescribing then, can enable “good deaths” to occur in accordance with patient and family wishes.
DISCUSSION
The relevance of international studies for the New Zealand context of community palliative care needs to be considered on various levels. At the most fundamental level, the relevance of anticipatory prescribing is universal, and indeed ethical. The definition and purpose of anticipatory prescribing – that palliative and end-of-life patients in physical distress should not have to wait for relief – remains the same.
Conceptually then, the principles underpinning anticipatory prescribing are universal. However, on a cultural level there are differences between palliative care in New Zealand and in other countries. Despite the cultural diversity that exists in the UK and Australia, through immigration and asylum, and the indigenous populations that live in Australia, culturally safe practices were not discussed in the articles reviewed. In New Zealand, considerable efforts have been put into developing culturally safe practices, particularly for Māori, the indigenous people of New Zealand. Health inequities have persisted for Māori for generations (MoH, 2020a; MoH & University of Otago, 2006), and a commitment to changing these inequities has shaped the education of health-care professionals in New Zealand, underpinned by the Treaty of Waitangi. Relating the concept of cultural safety to the findings of this study, the skills and competencies required for culturally safe practice fit with the “expertise” theme. As health-care professionals become more aware of the impact of their own views and biases (Medical Council of New Zealand, 2020), and seek to work with patients and whānau and their differing worldviews, the aim of achieving toi ora (health) could be closer to being realised (Te Rūnanga Hauora Māori o Te Moana a Toi, 2019).
The interdisciplinary approach encouraged by the Gold Standards Framework (2019) speaks to the value of different health professionals playing their part as a team in providing palliative care. Hierarchical attitudes and poor understandings of other professionals’ roles exist in New Zealand as well as overseas (Forgues, 2018). The primary care funding model in New Zealand may reinforce these attitudes and prevent more interdisciplinary approaches from occurring (Pullon et al, 2009). The fee-for-service model links payments to tasks, which separates the team into practitioner types, and the biggest revenue stream by far is for the doctors, who tend to work independently (Pullon et al, 2009). This model provides little incentive for a one-team approach in a context where privately-owned practices have fiscally tight margins and alternative ways of working may offer little guarantee of investment return. As for GPs having an interdisciplinary approach with other health professionals outside their practice, such as district nurses and ambulance personnel, the barriers are potentially greater, due to tight scheduling templates, and separate working facilities.
The professional scope of nurses in primary care has been much slower to advance in New Zealand than it has in the UK (Hoare et al, 2012). Community nurses have been able to prescribe injectable medications for end-of-life care since 1994 in the UK (Legislation UK, 1992), and as Bowers and Redsell (2017) reported, these nurses are frequently involved in initiating anticipatory prescribing. Twenty-seven years on, nurse prescribers in New Zealand still cannot prescribe injectable medications for palliative and end-of-life care (New Zealand Legislation, 2016; Nursing Council of New Zealand, 2018). Nurse practitioners working in primary care in New Zealand are able to attend to these end-of-life needs however, including for the anticipatory prescribing approach, and the numbers of these primary nurse practitioners are increasing (MoH, 2020b).
Members of the health workforce who provide palliative and end-of-life care will vary between the UK and New Zealand; indeed this varies within regions of New Zealand. When anticipatory medications are prescribed, it could vary from area to area who would administer them. District nurses, hospice nurses, doctors or ambulance personnel are the most likely members of the workforce to do this. Sometimes family members may be comfortable with carrying this out. Ambulance personnel have an increasing role in end-of-life care, particularly when families need support in the home at relatively short notice and when someone from their primary health-care team is not available (McCormick & Thompson, 2019).
Until now in New Zealand, anticipatory prescribing has featured more in specialised and residential care settings (Canterbury District Health Board, 2011; MoH, 2009; MoH, 2013), with little evidence of it being used in primary care. In the last few years however, the Te Ara Whakapiri documents Principles and Guidance for the Last Days of Life (MoH, 2017a) and Te Ara Whakapiri Toolkit Care in the Last Days of Life (MOH, 2017b) have encouraged anticipatory prescribing as a means of guiding the care of dying patients across all settings in New Zealand, including the home setting (MoH, 2017b). These documents view anticipatory prescribing as integral to planning for end-of-life care needs, responding quickly to symptoms and optimising the care that is delivered. General practice was also represented in the working group for these documents (MoH, 2017a).
LIMITATIONS
Most of the studies included in the meta-synthesis were from the UK, with just one from Australia. The limited availability of New Zealand research on anticipatory prescribing reduces the potential for broader insights. Studies which did not have an English translation were also excluded. Perhaps the most significant issue and limitation emerging from the selected studies, however, was that there was minimal consideration for cultural needs and equitable health care. Although cultural components of the UK and Australia have differences to New Zealand, it would have been useful to have diversity and equity incorporated in the thematic findings of the study.
CONCLUSIONS
This meta-synthesis has revealed that the factors which influence anticipatory prescribing in community palliative and end-of-life care settings fall under the themes of expertise, teamwork and prioritisation. Authorised prescribers require expertise in knowing when and how to prescribe anticipatory medications. Possessing the expertise to initiate and guide serious conversations with patients and whānau/family also promotes the anticipatory prescribing approach. It is readily apparent that a wider team is needed for an optimal anticipatory prescribing approach. An interdisciplinary approach can enable safer and more comprehensive palliative care to be provided, and is facilitated through a clear understanding of differing roles, open communication, relationship, trust and mutual respect. Finally, clinicians need to recognise the benefits of anticipatory prescribing given the unpredictable nature of end-of-life care, and take steps to prioritise it. If anticipatory prescribing is not prioritised, it potentiates patient and family crises, preventable access to and demand for acute services, and ultimately “bad deaths” for these patients and their whānau/families. Limiting the palliative prescribing approach to immediate indications rather than the likely and inevitable symptomatic needs will allow harm and inequities to continue. Anticipatory prescribing should therefore be enabled and embraced whenever possible and appropriate, to provide timely palliative and end-of-life care for patients and their whānau/families, supported by an interdisciplinary workforce.
RECOMMENDATIONS
- Education on anticipatory prescribing needs to be available to prescribers to equip them with the knowledge and skill to do this well, incorporating cultural safety and patient-centredness.
- Interdisciplinary training and education sessions are needed to foster teamwork in the provision of anticipatory prescribing.
- Experienced palliative care clinicians need to be retained to help upskill the existing workforce to be competent in improving timely palliative care in a patient-centred way.
- A nationally adopted tool is needed to improve consistency and equity in palliative care, either using the Supportive & Palliative Care Indicators Tool (SPICT) or the Gold Standard Framework (GSF), as determined through a consultation process.
- New Zealand research is urgently needed to understand the perspectives of patients and their whānau/family regarding anticipatory prescribing.
- Anticipatory prescribing could be added to the nurse prescribing scope in New Zealand, drawing on the experiences of nurses in the UK.
REFERENCES
Antunes, B., Bowers, B., Winterburn, I., Kelly, M. P., Brodrick, R., Pollock, K., Majumder, M., Spathis, A., Lawrie, I., George, R., Ryan, R., & Barclay, S. (2020). Anticipatory prescribing in community end-of-life care in the UK and Ireland during the COVID-19 pandemic: Online survey. British Medical Journal Supportive & Palliative Care, 10, 343–349.
Archer, M., Bhaskar, R., Collier, A., Lawson, T., & Norrie, A. (2013). Critical realism. Routledge.
Bhaskar, R. (1975). A realist theory of science. York Books.
Bowers, B., Barclay, S. S., Pollock, K., & Barclay, S. (2020). GPs’ decisions about prescribing end-of-life anticipatory medications: a qualitative study. British Journal of General Practice: The Journal of the Royal College of General Practitioners, 70(699), e731–e739.
Bowers, B., & Redsell, S. A. (2017). A qualitative study of community nurses’ decision-making around the anticipatory prescribing of end-of-life medications. Journal of Advanced Nursing, 73(10), 2385–2394.
Brady, M. (2016). Care of dying adults in the last days of life: NICE clinical guideline. Journal of Paramedic Practice, 8, 63-65.
Broad, J. B., Ashton, T., Gott, M., McLeod, H., Davis, P. B., & Connolly, M. J. (2015). Likelihood of residential aged care use in later life: a simple approach to estimation with international comparison. Australian and New Zealand Journal of Public Health, 39(4), 374-379.
Brown, M. (2015). Palliative Care in Nursing and Healthcare. (pp. 76-90). SAGE Publications Ltd.
Bygstad, B., Munkvold, B. E., & Volkoff, O. (2016). Identifying Generative Mechanisms through Affordances: A Framework for Critical Realist Data Analysis. Journal of Information Technology, 31(1), 83–96.
Canterbury District Health Board. (2011, May). Anticipatory prescribing for patients with a terminal illness: “Just in case”. CDHB Palliative Care Service.
Chakravartty, A. (2017). Scientific realism. Stanford Encyclopaedia of Philosophy.
Dyess, S. M., Prestia, A. S., Levene, R., & Gonzalez, F. (2020). An interdisciplinary framework for palliative and hospice education and practice. Journal of Holistic Nursing, 38(3), 320–330.
Eastwood, J. G., Jalaludin, B. B., & Kemp, L. A. (2014). Realist explanatory theory building method for social epidemiology: A protocol for a mixed method multilevel study of neighbourhood context and postnatal depression. Springer Plus, 3, 12.
Faull, C., Windridge, K., Ockleford, E., & Hudson, M. (2013). Anticipatory prescribing in terminal care at home: What challenges do community health professionals encounter? BMJ Supportive & Palliative Care, 3(1), 91–97.
Forgues, I. (2018). Barriers and facilitators to RN-GP communication in aged residential care in the South Island, New Zealand.
General Medical Council. (2021). Good practice in prescribing and managing medicines and devices.
Gold Standards Framework. (2019). What we do: Update from the GSF Centre 2019.
Grattan Institute. (2014, September). Dying Well.
Health Quality & Safety Commission. (2020). National summary of adverse events reported to the Health Quality & Safety Commission 1 July 2019 to 30 June 2020.
Hoare, K. J., Mills, J., & Francis, K. (2012). The role of Government policy in supporting nurse-led care in general practice in the United Kingdom, New Zealand and Australia: An adapted realist review. Journal of Advanced Nursing, 68(5), 963–980.
Joanna Briggs Institute [JBI]. (2017). Critical Appraisal Tools. Checklist for Qualitative Research.
Khalil, H., Garett, M., Byrne, A., Poon, P., Gardner, K., Azar, D., Craig, L., & Karimi, L. (2021). Mapping end-of-life and anticipatory medications in palliative care patients using a longitudinal general practice database. Palliative and Supportive Care, 1-7.
Kidd, J., Black, S., Blundell, R., & Peni, T. (2018). Cultural health literacy: The experiences of Mâori in palliative care. Global Health Promotion, 25(4), 15-23.
Lawton, S., Towsey, L., & Carroll, D. (2013). What is a “good death” in the care home setting? Nursing and Residential Care, 15(7), 494-497.
Legislation UK. (1992). Medicinal Products: Prescription by Nurses etc. Act 1992.
McCormick, G., & Thompson, S. (2019). The provision of palliative and end-of-life care by paramedics in New Zealand communities: A review of international practice and the New Zealand context. Whitireia Journal of Nursing, Heath and Social Services, 26, 51–57.
McLeod, H. (2016, June). The Need for Palliative Care in New Zealand. Technical Report: Need for Palliative Care.
Medical Council of New Zealand Te Kaunihera Rata o Aotearoa. (2020, October). Statement on cultural safety.
Ministry of Health/Manatū Hauora & University of Otago. (2006). Decades of disparity III: Ethnic and socioeconomic inequalities in mortality, New Zealand 1981-1999. Public Health Intelligence Occasional Bulletin No.31.
Ministry of Health [MoH]. (2009). Guidelines for Syringe Driver Management in Palliative Care in New Zealand.
Ministry of Health [MoH]. (2011, September). Palliative care.
Ministry of Health [MoH]. (2012). Resource And Capability Framework For Integrated Adult Palliative Care Services In New Zealand.
Ministry of Health [MoH]. (2013). Medicines Management Guide For Community Residential And Facility-Based Respite Services: Disability, Mental Health And Addiction.
Ministry of Health [MoH]. (2014). Palliative Care and Māori from a Health Literacy Perspective.
Ministry of Health [MoH]. (2016). New Zealand Health Strategy: Roadmap of Actions 2016.
Ministry of Health [MoH]. (2017a). Te Ara Whakapiri: Principles and guidance for the last days of life.
Ministry of Health [MoH]. (2017b). Te Ara Whakapiri Toolkit: Care in the last days of life.
Ministry of Health [MoH]. (2019). Achieving Equity In Health Outcomes: Highlights Of Important National And International Papers.
Ministry of Health [MoH]. (2020a). Whakamaua Māori Health Action Plan 2020–2025.
Ministry of Health [MoH]. (2020b). Nurse practitioners in New Zealand.
National Clinical Guideline Centre. (2015, December). Care Of Dying Adults In The Last Days Of Life (NICE Guideline 31). National Institute for Health and Care Excellence.
New Zealand Legislation. (2016). Medicines (Designated Prescriber – Registered Nurses) Regulations 2016.
Nilsson, J., Blomberg, C., Holgersson, G., Carlsson, T., Bergqvist, M., & Bergström, S. (2017). End-of-life care: Where do cancer patients want to die? A systematic review. Asia-Pacific Journal of Clinical Oncology, 13(6), 356-364.
Nursing Council of New Zealand. (2018). Tapuhi tūtohu kua rēhitatia Registered Nurse Prescribing.
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., McGuinness, L. A., Stewart, L. A., Thomas, J., Tricco, A. C., Welch, V. A., Whiting, P., & Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Systematic Reviews, 10, 89.
Palliative Care Council of New Zealand (2010, February). Positioning Palliative Care In New Zealand: A review of government health policy in relation to the provision of palliative care services in New Zealand.
Pennec, S., Gaymu, J., Riou, F., Morand, E., Pontone, S., Aubry, R., & Cases, C. (2015). A majority of people would prefer to die at home, but few actually do so. Population & Societies, 7(7), 1-4.
Power, J., Gilmore, B., Vallières, F., Toomey, E., Mannan, H., & McAuliffe, E. (2019). Adapting health interventions for local fit when scaling-up: A realist review protocol. BMJ Open, 9.
Pullon, S., McKinlay, E., & Dew, K. (2009). Primary health care in New Zealand: The impact of organisational factors on teamwork. British Journal of General Practice, 59(560), 191–197.
Rome, R. B., Luminais, H. H., Bourgeois, D. A., & Blais, C. M. (2011). The role of palliative care at the end of life. Ochsner Journal, 11(4), 348–352.
Spacey, A., Scammell, J., Board, M., & Porter, S. (2019). Systematic critical realist review of interventions designed to improve end-of-life care in care homes. Nursing & Health Sciences, 22(2), 343–354.
Stanford School of Medicine. (2021). Palliative Care: Where do Americans die?
Stenner, K., & Courtenay, M. (2008). The role of inter-professional relationships and support for nurse prescribing in acute and chronic pain. Journal of Advanced Nursing, 63, 276-83.
Stevens, A. (2020). Critical realism and the “ontological politics of drug policy.” International Journal of Drug Policy, 84.
Te Rūnanga Hauora Māori o Te Moana a Toi. (2019). Te Toi Ahorangi: Te Rautaki a Toi Ora 2030. Law Creative.
Thomas, K., & Noble, B. (2007). Improving the delivery of palliative care in general practice: An evaluation of the first phase of the Gold Standards Framework. Palliative Medicine, 21(1), 49-53.
Thomas, K., Armstrong Wilson, J., & GSF Team. (2016). The GSF Prognostic Indicator Guidance: The National GSF Centre’s guidance for clinicians to support earlier recognition of patients nearing the end of life leading to improved proactive person-centred care (6th ed.).
Wilson, E. & Seymour, J. (2017). The importance of interdisciplinary communication in the process of anticipatory prescribing. International Journal of Palliative Nursing, 23(3), 129-135.
Wilson, E., Seymour, J., & Seale, C. (2016). Anticipatory prescribing for end-of-life care: A survey of community nurses in England. Primary Health Care, 26(9), 22-27.
World Health Organization. (2020, August). Palliative Care.
Daily doses – uncut news
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


