
About the authors:William Chiyesu, RN, RM, DipNursing, MHSc, is a clinical nurse specialist in the respiratory service, Counties Manukau Health, Auckland, New Zealand. Shayne Rasmussen, RN, MHSc(hons), is a nursing lecturer at the Auckland University of Technology. This article was accepted for publication in September 2021. |
ABSTRACTAim: To explore whether the education component in a pulmonary rehabilitation programme (PRP) influences health outcomes for chronic obstructive pulmonary disease (COPD) patients. Methodology: An integrative review of literature was employed in the study to allow for narrative integration of results from qualitative, quantitative and mixed-methods articles. Findings: The research findings from 11 reviewed articles highlighted the following concepts: “Knowledge of the disease”, “knowledge as key to self-management” (with sub-concepts “management of symptoms” and “management of psychosocial symptoms”) and “the relationship between knowledge and education”. Discussion: Insufficient evidence exists about the importance of education in PRPs. Therefore, health practitioners providing PRPs must consider, as standard practice, evaluating the educational component to highlight evidence of its significance. Conclusion: The educational component of PRPs for people with COPD is not currently supported by sufficient evidence showing its influence on health outcomes. Robust research is required to investigate the influence of the educational component of PRPs in any setting and to test a suitable measurement tool on people with COPD in New Zealand. Further research is required to evaluate the teaching methods currently being used in any PRP settings where cultural diversity is prominent in New Zealand. This should investigate the relevance of the topics being covered in the current education component from the patient’s perspective, and explore the involvement of cultural leaders/peer groups in the delivery of education. |
||
KEYWORDSpulmonary rehabilitation programme, education, COPD, knowledge, self-management |
|||

INTRODUCTION
A PULMONARY REHABILITATION PROGRAMME (PRP) is a comprehensive non-pharmaceutical intervention. It includes thorough patient assessment and individually-tailored therapies, such as exercise training, education and self-care interventions aimed at lifestyle changes to improve health (Nici et al., 2009; Paneroni et al., 2013; Zeng et al., 2018). These programmes are intended to improve the physical and psychological well-being of people with chronic obstructive pulmonary disease (COPD) and to promote long-term adherence to health-enhancing behaviours (Global Initiative for Chronic Obstructive Lung Disease [GOLD], 2019). International and national guidelines stipulate that exercises and education are the two core elements of PRP.
Exercise interventions have traditionally been the role of physiotherapists. However, in New Zealand, respiratory nurses can lead and support PRPs. Respiratory nurses work alongside the respiratory physiotherapist to provide a complete PRP package which includes providing education. Respiratory nurses are responsible for assessing, developing nursing plans and screening patients appropriate for PRP, as guided by GOLD (2019).
There are evidence-based recommendations for the exercise component, including the prescription of exercises; however there is no unequivocal scientific evidence on the real learning benefit from a single educational approach in patients with COPD (Crisafulli et al., 2010; Wilson et al., 2007). Participants in previous studies expressed dissatisfaction with their knowledge about COPD (Casey et al., 2011; Sandelowsky et al., 2019), and the development of the educational component has been highlighted as a significant area for research (National Collaborating Centre for Chronic Conditions, 2004).
SIGNIFICANCE OF THE STUDY
COPD is a common, preventable disease characterised by persistent respiratory symptoms and airflow limitations due to airway and/or alveolar abnormalities, usually caused by significant exposure to noxious particles or gases (GOLD, 2019; Vestbo et al., 2013). It is a wide-spectrum disorder, which includes chronic bronchitis and emphysema. The consequences of COPD are usually noticed in people in their late 40s (GOLD, 2019). The number of people with COPD worldwide is expected to rise over the next 30 years due to continued exposure to COPD risk factors and the numbers of people of low socioeconomic status. It is the third leading cause of death worldwide and by 2030, the annual death toll is expected to be 4.5 million (GOLD, 2019; Vestbo et al., 2013).
COPD in New Zealand
New Zealand has one of the highest rates of COPD cases in Organisation for Economic Co-operation and Development (OECD) countries (Milne & Beasley, 2015). Milne and Beasley’s (2015) study showed that COPD was a major health problem in New Zealand, reflected in high numbers of hospital admissions. In the year 2012/13, there were 12,418 admissions with a principal diagnosis of COPD. The cost per admission was estimated at NZ$4799, costing district health boards (DHBs) a total of NZ$59.59 million in 2012/13 (Milne & Beasley, 2015).
In New Zealand, Māori were reported to have the highest rate of COPD mortality, with 190.7 deaths per 100,000 people per year, which is 2.24 (95% CI 2.04-2.41) times higher than the rate of 85.1 for non-Māori, Pacific and Asian people (Telfar Barnard & Zhang, 2016). COPD is the fourth leading cause of mortality in New Zealand (Milne & Beasley, 2015). The hospital admission rate for Māori is double that of non-Māori but the degree to which this represents a greater COPD incidence among Māori is not known (Milne & Beasley, 2015).
There is a direct relationship between the severity of COPD and the cost of care (Milne & Beasley, 2015). The huge cost spares neither the public health system nor individual patients and their families – eg the cost of hospitalisation and of ambulatory oxygen increase as COPD severity progresses.
Factors leading to high rates of hospital admission include lower socioeconomic status, exposure to smoking, and geographical location. Māori and Pacific people have a higher chance of exposure to the risk factors of COPD, leading to higher rates of hospital admission (Milne & Beasley, 2015). In part, this may be a result of delays in seeking medical help and the variation in care delivered in different settings, especially in rural areas, reflecting inequity in health services (Milne & Beasley, 2015). Telfar Barnard and Zhang (2016) state that COPD mortality rates are directly proportionate to socioeconomic deprivation, with deaths in the NZDep2006 quintile 9-10 (the most deprived) occurring at 2.37 times the rate in quintile 1-2 (the least deprived) (per Figure 65 in Telfar Barnard & Zhang, 2016).
SIGNIFICANCE OF PULMONARY REHABILITATION PROGRAMMES
Alison et al. (2017) stated that attendance at PRPs for people with COPD improved exercise tolerance and health-related quality of life, and reduced hospitalisation. The PRP has proved to be an effective intervention in improving shortness of breath for COPD patients (GOLD, 2018). Pulmonary rehabilitation ranks as one of the most cost-effective treatment strategies, with an estimated cost per quality-adjusted life years of NZ$2000-NZ$8000 (GOLD, 2018).
Blackstock et al. (2014) argued that the benefits directly attributed to the education component remain unclear. These authors further stated that pulmonary rehabilitation education has not been evaluated or clearly defined. There is currently insufficient validated research internationally to demonstrate the importance of the educational programme for COPD patients. There has not been a specific study which has evaluated the role of the educational component without including exercises (Blackstock et al., 2014). Therefore, it is unclear whether any benefits gained by COPD patients which enhance health behaviours, leading to better health-related quality of life, are a result of physical exercise or education (Blackstock et al., 2014).
Current practice models recommend evaluation of improvements in patients’ health status and exercise capacity after pulmonary rehabilitation, but the assessment of the educational component is not routine practice (Jones et al., 2008). Jones et al. suggest that COPD knowledge questionnaires are too long and reflect the health-care professional’s perspective rather than that of the patient. In addition, there have been no validated tools developed to assess the benefits gained from the educational component of PRP for people with COPD (O’Neill et al., 2012; White et al., 2006).
The purpose of this study is to explore whether the education component in PRPs influences health outcomes for patients with COPD.
METHODOLOGY
An integrative review of results from qualitative, quantitative and mixed-methods research (Whittemore & Knafl, 2005) was undertaken, specifically focused on education of people with COPD. Integrative reviews are broadly used to provide an auditable and robust synthesis of qualitative, quantitative and mixed-methods literature to construct new knowledge (Brady et al., 2019; Neville et al., 2016; Wright-St Clair et al., 2017). Quantitative, qualitative and mixed-methods perspectives are informative when seeking to answer empirical and theoretical research questions.
Philosophical perspective
This integrative review is underpinned by the philosophical dimensions of a post-positivistic approach in which it is argued that there is no best design in developing knowledge, and no reason to assume that qualitative and quantitative methods are incompatible. It allows for the application of diverse methodologies to develop knowledge of a phenomenon (Houghton, 2011). Houghton contended that claims about knowledge must be subjected to wide critical scrutiny to help to expose reality as closely as possible. Post-positivism acknowledges that the outcome of an investigation is an estimation of the truth, rather than truth itself (Grove & Gray, 2018).
METHODS
The specific techniques and procedures for literature search and data analysis were guided by Whittemore and Knafl’s (2005) conceptual framework, which offers a rigorous process for the integrative review of relevant literature. The process follows these five stages:
(1) Problem identification, which ensures the research question and its purpose are clearly defined.
(2) Literature search, which incorporates a comprehensive search strategy.
(3) Data evaluation, which focuses on the authenticity, methodological quality, informational value and representativeness of available primary studies.
(4) Data analysis, which includes data reduction, display, comparison and conclusion.
(5) Presentation, which synthesises findings in a model that comprehensively portrays the integration process and describes the implications for practice, policy and research as well as the limitations of the review.
Hopia et al. (2016) appraised the integrative review process to consolidate the methodological approach in accordance with the five stages published by Whittemore and Knafl (2005).
For this study, a comprehensive approach to the search strategy was designed with the support of an experienced librarian, and used electronic academic databases. The databases included: Cumulative Index to Nursing and Allied Health Literature (CINAHL), Medline, PubMed, Scopus and Google Scholar.
Keywords employed in the search strategy were: “COPD”, “integrative review”, “pulmonary rehabilitation programme”, “education”, “evaluation/assessment tools”, “outcome measure*”, “self-reporting questionnaire”, “psychometric properties” and “measurement tools”. Truncations (*) were employed to include spelling variations or similar terms.
Inclusion criteria
Inclusion criteria for the search included peer-reviewed articles using the keywords mentioned above. Only articles in English were reviewed and citation-index searching, which involved references used in published articles, was used. The citation index is highly recommended because it is based on the citing practices of authors, who commonly refer to studies similar to the original citation (Conn et al., 2003). Other high-quality articles on education for COPD patients were considered, including those on the development of structured education programmes for people with a confirmed diagnosis of COPD only. Peer-reviewed articles published in the years 2000 to 2020 were included. To ensure rigour, the peer-reviewed articles were screened by the second author and confirmed for inclusion.
Exclusion criteria
Excluded from this integrative literature review were studies on education for asthma or other chronic airways diseases. One study by Terwee et al. (2007), who outlined a measurement of the properties of a health status questionnaire, was excluded because it was not specifically on COPD.
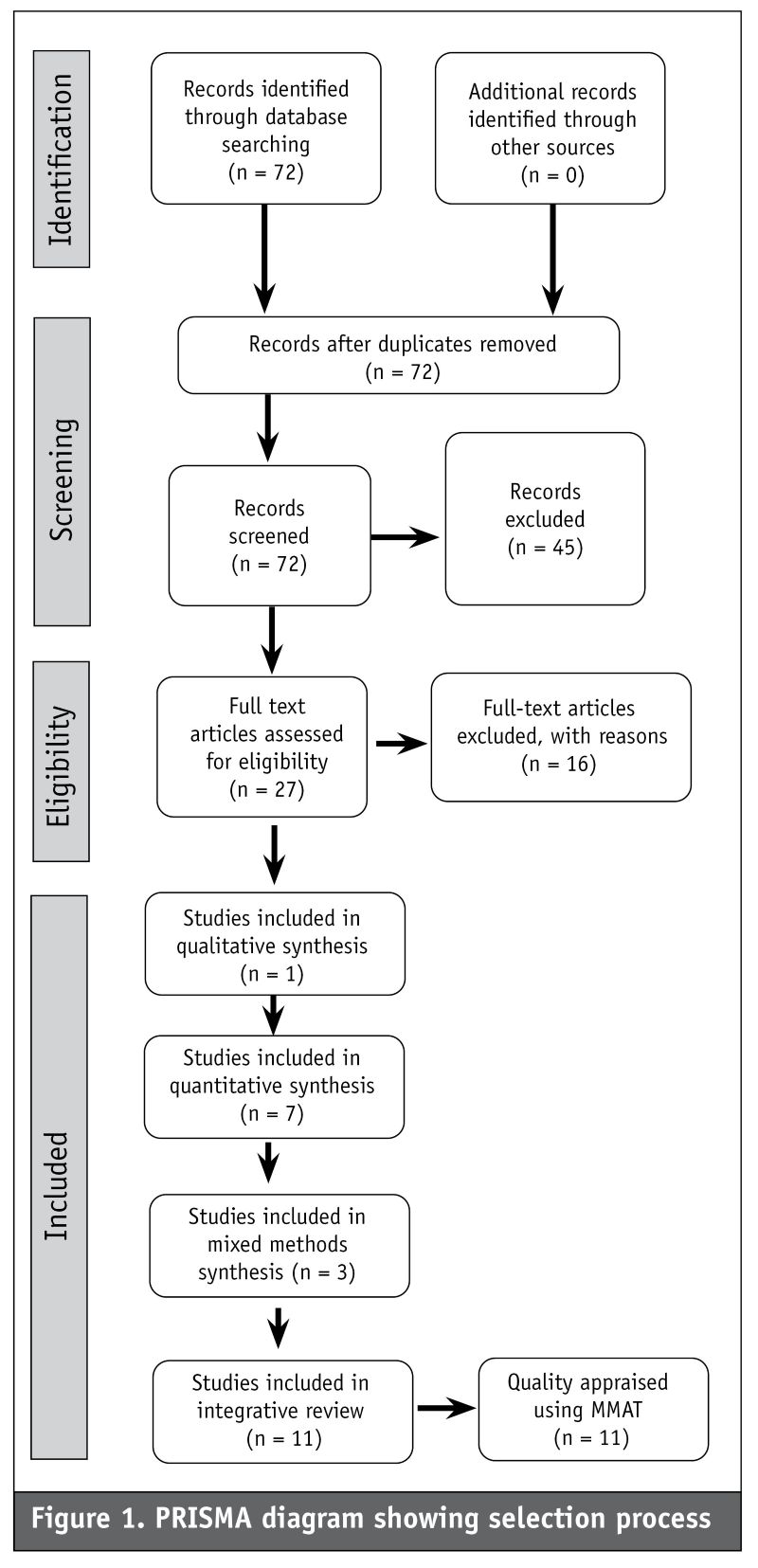
An outline of the search results is displayed in the Preferred Reporting Item for Systematic reviews and Meta-Analysis (PRISMA) diagram, shown in Figure 1 (below). Through the reading and re-reading of the articles’ abstracts and full text to ensure the evidence was relevant to the topic, the selected literature was reduced to n=11 articles to be synthesised in this integrative review.
Quality evaluation
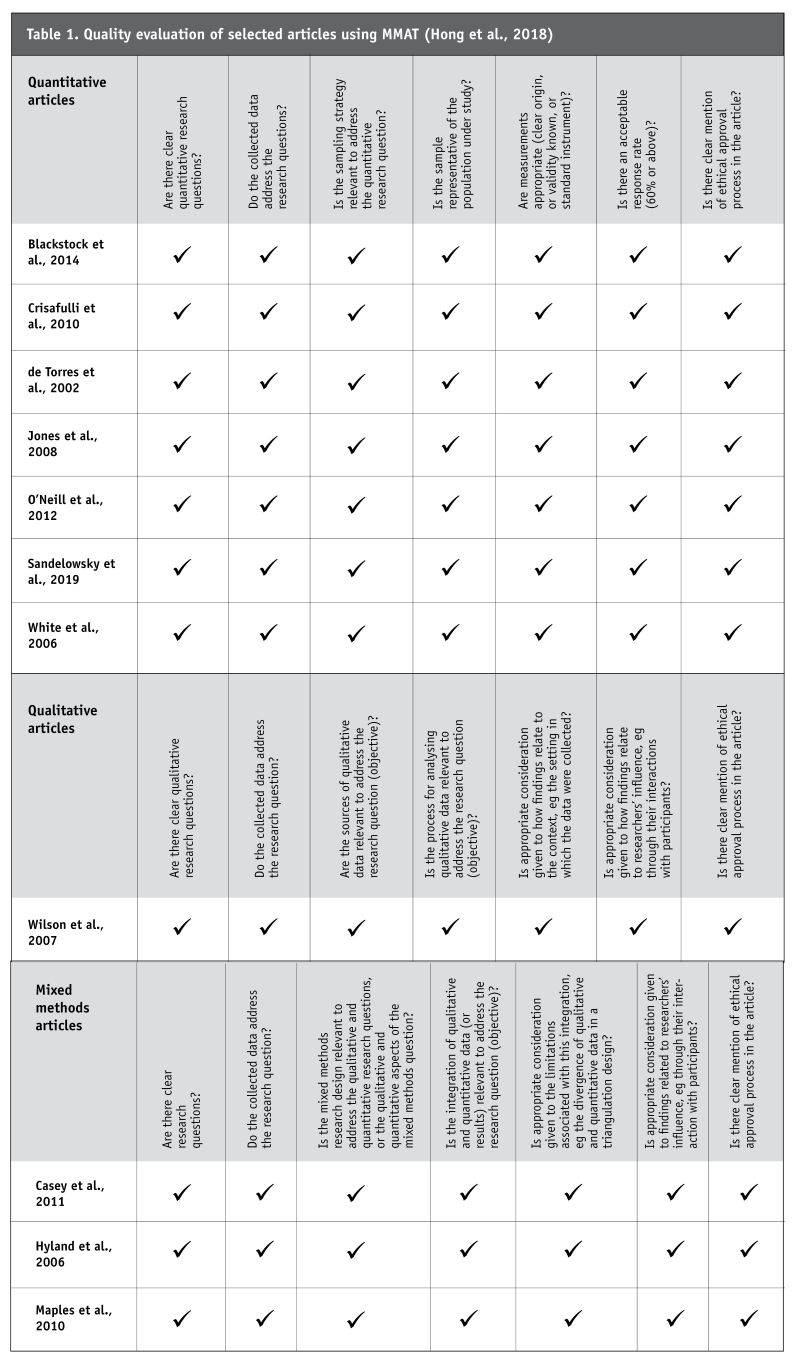
The quality appraisal tool Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018) was applied to assess the methodological quality of the studies included. After applying the MMAT screening questions (see Table 1 below), the conclusion was that all 11 studies included in the review were methodologically reliable and met the quality appraisal criteria.
Ethics
All studies included in the integrative review noted ethical approval.
Data analysis
Eligible articles were read and re-read to work out the key patterns in the primary data. Through an iterative process, headings were conceptualised by re-grouping similar data under the headings, following Whittemore and Knafl’s (2005) elements of data analysis. These elements are: noting patterns, seeing plausibility, clustering, contrasting and comparing data. The results from the 11 eligible studies were then integrated, synthesised and conceptualised to interpret the data.
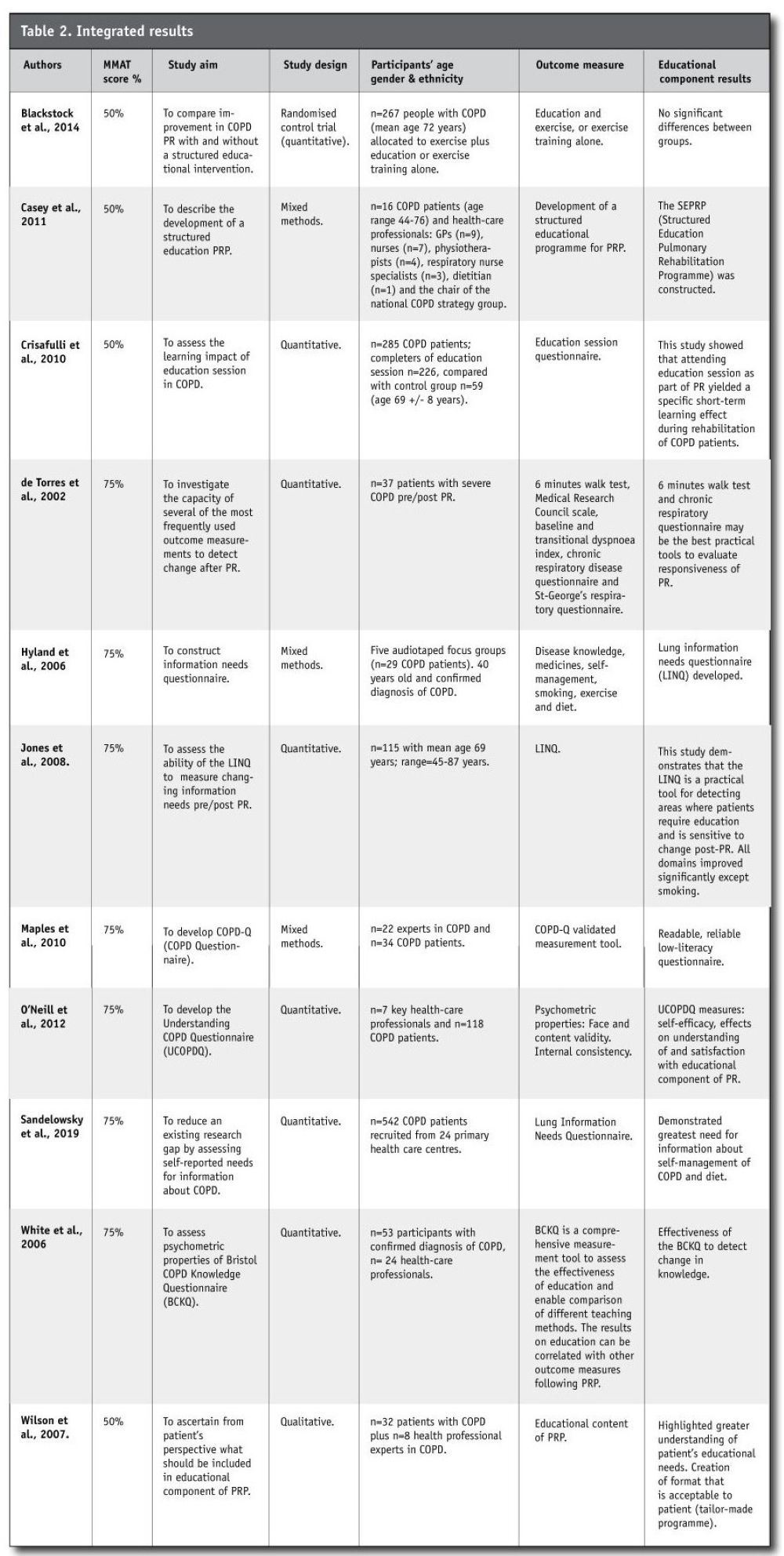
The 11 eligible studies consisted of: seven quantitative studies with a total of 865 participants – this demonstrates a significant number of participants capable of providing robust results; only one qualitative study, which involved 32 participants; and three mixed-methods studies, which recruited a total of 943 participants. The data characteristics of the articles are summarised in Table 2.
RESULTS
Data characteristics
The studies reported in the 11 included articles were conducted in various countries. Six were from the United Kingdom, one from Italy, one from Sweden, one from Australia and two from the United States.
The 11 articles employed diverse methodologies, namely: quantitative (Blackstock et al., 2014; Crisafulli et al., 2010; de Torres et al., 2002; Jones et al., 2008; O’Neill et al., 2012; Sandelowsky et al., 2019; White et al., 2006); qualitative (Wilson et al., 2007); and mixed methods (Casey et al., 2011; Hyland et al., 2006; Maples et al., 2010).
All 11 articles included in the review were peer-reviewed and reliable. The ages of participants in the studies ranged from 49 to 86 years, which reflects the fact that symptoms of COPD manifest later in life (White et al., 2006). Both male and female genders were included in the 11 studies. The study sizes ranged from Wilson et al. (2007), with n=32, up to Hyland et al. (2006) which had the highest number of participants at n=590.
Data conceptualisation
The data from the studies was summarised and then organised into conceptual categories. Using an iterative approach, this data was eventually consolidated under headings and sub-headings to compare differences and similarities in the 11 articles. The following headings and sub-headings were developed as conceptual terms from the results: Knowledge of the disease; knowledge as key to effective self-management (with sub-headings for management of symptoms and management of psychosocial symptoms); and relationship between knowledge ↔ education. These three data conceptualisations covered all studies and incorporated the key findings.
Knowledge of the disease
A key conceptual finding in the reviewed data was COPD patients’ knowledge of the disease, which promotes independent self-care (Casey et al., 2007; Maples et al., 2010; O’Neill et al., 2012; Sandelowsky et al., 2019; White et al., 2006; Wilson., 2007). For example, participants in one study reported “knowing own norms and limits”, “knowing when you are in trouble”, “knowing what to do”, and “but I do find when I get the niggling pain in my left lung and sputum changes colour, that I know I’m getting an infection” (Casey et al., 2011, p. 184). These participants demonstrated pre-existing knowledge and skills for self-management. In contrast, Wilson et al. (2007) argued that there were consistencies in results demonstrating lack of knowledge across all participants in the domain of diagnosis and continued care.
Sandelowsky et al. (2019) suggested that people with moderate COPD who had chest infections reported a significantly higher need for information than those with severe disease. However, people with severe disease were highly likely to demonstrate higher levels of knowledge because of several encounters with health-care professionals (Sandelowsky et al., 2019). In contrast, White et al. (2006) suggested “age, socioeconomic status and disease severity did influence the degree of knowledge” (p. 129) in people with COPD. They further suggested that a significant proportion of participants had inaccurate knowledge about COPD and that it might be difficult to accurately ascertain people’s knowledge, even using verified tools, where factors other than knowledge shaped behavioural responses (White et al., 2006).
Knowledge as a key to effective self-management
Many of the studies highlighted the importance of knowledge and understanding if people with COPD were to effectively manage their own health and well-being. Understanding of one’s body was important to adapting health behaviour to improve the quality of life (Casey et al., 2011; Hyland et al., 2006; White et al., 2006; Wilson et al., 2007). The application of knowledge about COPD by individuals and families can be regarded as effective self-management strategies. For instance, Casey et al. (2011) stated that participants acknowledged that the provision of information and knowledge related to COPD was important for enhancing self-management.
The results from the studies by Crisafulli et al. (2010), Hyland et al. (2006), Jones et al. (2008), O’Neill et al. (2012), Sandelowsky et al. (2019) and Wilson et al. (2007) showed that knowledge was the key to self-management. Wilson et al. (2007) had similar results, demonstrating that knowledge about pulmonary conditions could influence patients’ behaviour in managing their symptoms. Crisafulli et al. (2010) stated that COPD patients’ knowledge contributed substantially to reduced hospital admission rates, and that they retained knowledge over two years. For instance, education session total and partial scores significantly changed (p=0.001) for participants who completed pulmonary rehabilitation (Crisafulli et al., 2010).
Self-management is a key concept in the care of people with chronic conditions worldwide. Self-management is defined in the reviewed literature as the ability of people with chronic conditions to apply acquired knowledge and skills to independently self-care (Blackstock et al., 2014; Crisafulli et al., 2010; Jones et al., 2008). However, Sandelowsky et al. (2019) found that participants lacked knowledge about diet and self-management, highlighting the need to provide education on COPD related to nutrition and self-care.
The following sub-sections separate findings on the management of symptoms from those on the management of psychosocial symptoms.
Management of symptoms: Some of the studies (Casey et al., 2011; Crisafulli et al., 2010; Sandelowsky et al., 2019; Wilson et al., 2007) demonstrated that early recognition of the signs and symptoms of an exacerbation of the disease, and being able to navigate support through health-care services, is significant for self-management. It is through exposure to the educational component of a PRP that people with COPD acquire the knowledge and skills to self-administer these therapeutic interventions without daily supervision by health-care professionals. For example, participants in Casey et al.’s (2015) study recognised changes in their bodies “and straight away I act by ringing the team and going into hospital” (p. 184). Crisafulli et al. (2010) stated that education led to a substantial reduction in hospitalisation rates over a period of two years. Despite self-management being key to managing chronic conditions, the concept often takes a narrow focus of recognising the signs and symptoms of an exacerbation of COPD. Other strategies also need to be included for holistic care (Jones et al., 2008; Sandelowsky et al., 2019).
Management of psychosocial symptoms: Knowledge as a key to self-management will be incomplete if other disabilities which manifest as a result of chronic illness are not considered. Some of the studies identified anxiety and depression as correlated with COPD; increased knowledge, however, could help reduce anxiety and depression after exposure to pulmonary rehabilitation (Jones et al., 2008). Sandelowsky et al. (2019) found similar results, showing that lower levels of education about COPD were a significant risk factor for anxiety and depression. Therefore, addressing self-management should incorporate input from a health psychologist.
Knowledge ↔ education
The last data category is “knowledge ↔ education”. The symbol between the two words indicates there is a relationship between knowledge and education where each concept is distinct from the other while also related to the other. The relationship between education and knowledge is not static and assumptions that education improved knowledge were not substantiated.
Many clinicians believe that educating patients translates into the knowledge needed to make lifestyle changes and thus to improve health. However, the results demonstrate that knowledge and education may not be interpreted as the same thing (Maples et al., 2010; Sandelowsky et al., 2019; White et al., 2006). Maples et al. (2010) suggested that participants with or without prior knowledge of COPD scored similar post-intervention results (p>0.001). These studies demonstrated that even without exposure to an education intervention, people with a confirmed diagnosis of COPD had prior knowledge of the disease.
The data showed participants possessed knowledge even before any formal education through a PRP. Maples et al. (2010) suggested participants had prior knowledge about COPD on their first contact with health-care professionals in a PRP. Sandelowsky et al. (2019) showed that, in the domains of medication and smoking, participants demonstrated prior knowledge. However, while most participants had pre-existing knowledge on the effects of smoking, it was unclear whether participants had knowledge on smoking cessation. Knowledge can be acquired through lived experience or through an education programme related to a particular chronic condition (Sandelowsky et al., 2019). White et al. (2006), for example, showed that education related to COPD did lead to significant improvements in knowledge. Jones et al. (2008) demonstrated that education clearly improved knowledge in most domains except for smoking, on which participants had prior knowledge. Education related to COPD led to improved knowledge (White et al., 2006). However, Wilson et al. (2007) suggested that participants with COPD who engaged in pulmonary rehabilitation reported “dissatisfaction with COPD knowledge [and] were unclear about the aetiology of COPD” (p. 1706). This highlighted that improved knowledge is not the same as having adequate knowledge related to COPD. The comments quoted above referred to dissatisfaction following an education intervention in pulmonary rehabilitation, as opposed to being satisfied with their existing knowledge. It is unclear whether the results which captured this dissatisfaction with knowledge were incidental or reflected an inability by individuals to understand the educational content and the way it was delivered.
Findings from Hyland et al. (2006) showed participants were satisfied with the structure and process of the educational component of PRP, rather than their knowledge related to COPD. For example, 21 percent of the participants did not know the name of their disease, 3 percent reported non-compliance and 8 percent were confused about their inhalers. Despite participants attending an educational programme, they still had inaccurate knowledge about COPD. For instance, most respondents seemed to misunderstand the meaning of “chronic”, thinking it meant “severe” rather than “longterm” (White et al., 2006).
Researchers have applied validated measurement tools to demonstrate the place of exercise in PRP. Therefore, the significant impact of exercise in improved health outcomes must be accepted. For instance, O’Neill et al. (2012) applied UCOPD to demonstrate the efficacy of the educational component in PRP. Education informs pulmonary rehabilitation in the sense of creating an awareness of the benefits of the programme. It is at this stage of contact in PRPs that a measurement tool can be employed to inform the educational component of pulmonary rehabilitation with the information needs of people with COPD.
Sandelowsky et al. (2019) stated that participants (68 percent) who had no contact with health-care professionals had a high perceived need for information, unlike those who had contact with health-care professionals. These results showed that health-care professionals provided some form of information about COPD in each encounter, but it cannot be extrapolated to say how that occurs or whether the increased knowledge is adequate for COPD patients to effectively self-manage their health signs and symptoms.
DISCUSSION
There is insufficient evidence of the contribution made by the educational component of PRPs in New Zealand, when compared to the exercise component. This could partly be a result of insufficient research on validated assessment tools to evaluate the impact of the educational component (Blackstock et al., 2014; Crisafulli et al., 2010; White et al., 2006). Therefore, the place of the educational component of PRPs remains unclear. By comparison, in other chronic conditions such as diabetes mellitus and heart failure, education is known as the cornerstone of interventions to influence lifestyle changes for improved self-management (Peterson et al., 2011; Steinsbekk et al., 2012; Strömberg, 2005).
Knowledge of the disease
Health-care professionals have used the traditional didactic method of presenting information and advice to COPD patients, assuming that knowledge will enhance behavioural change (GOLD, 2018). Enhancing patients’ knowledge is a major step towards behaviour change (GOLD, 2018). Whether this knowledge translates into changed behaviour depends on the individual patient, the mode of delivery and the content of the education package (GOLD, 2018). However, the susceptibility of certain behaviour to being transformed must be assessed, and the impact of different theory-based educational techniques must be included to bring about the anticipated change (Harris et al., 2008). Education helps COPD patients to understand their chronic pulmonary condition and may increase their ability to take action to seek medical help in a timely manner (Omachi et al., 2013). Although pulmonary rehabilitation improves physical function, most studies did not show that education alone improved health-related quality of life (Blackstock et al., 2014; Monninkhof et al., 2003). Monninkhof et al. (2003) suggested that early education intervention with newly diagnosed COPD participants showed benefits in the self-management of their symptoms. There is, however, little evidence to suggest that knowledge is retained over time.
Knowledge as a key to effective self-management
Casey et al. (2011) suggested that participants acknowledged that accessing information and knowledge related to COPD was significant for promoting self-management. Crisafulli et al. (2010) highlighted that education was a precursor which substantially lessened hospital admissions in participants with COPD over a period of two years. Jones et al. (2008) argued that although participants showed no improvement in self-management after taking part in a PRP educational session, this was in part due to individual participants’ inability to acquire knowledge. Thus the health-care professionals needed to review the content and delivery of the educational intervention.
To provide holistic care to people with COPD, their physical and psychosocial symptoms need to be addressed. In the studies conducted by Jones et al. (2008) and Sandelowsky et al. (2019), the authors suggested a low level of COPD knowledge was associated with anxiety and depression. Anxiety and depression are common in people with COPD as the disease progresses (Gudmundsson et al., 2005). Although this was not the focus of the present study, these results showed that a lack of knowledge related to COPD predisposed respondents to scoring more in the domain of anxiety and depression. Jang et al. (2019) showed that the incidence of anxiety and depression was significantly reduced following short-term education, which encouraged awareness and advised on coping strategies.
Knowledge ↔ education
The conceptualisation of knowledge ↔ education reflects the fact that knowledge and education are evident in the data; however, they are correlated rather than equivalent. Past work experiences of health-care professionals suggested that any health education improved knowledge (White et al., 2006). This implies that participants with COPD had prior knowledge. However, education improved knowledge related to the disease. Jones et al. (2008) stated that education clearly improved knowledge, but not in the domain of smoking because participants had prior knowledge on smoking as a predisposing factor of COPD. Even if participants presented with pre-existing knowledge, this did not apply in all areas being measured. The uptake of information varied between individual patients and, as a result, some respondents scored high for non-medication related elements of self-management. Sandelowsky et al. (2019) also maintained that participants showed the least need for education in the areas of medication and smoking. This may suggest that health-care professionals provided more information on medication and smoking, compared to other aspects of self-management. White et al. (2006) further stated that, regardless of a participant’s involvement in the educational part of a PRP, they still had inaccurate knowledge about COPD. For example, the word “chronic” was interpreted by respondents as referring to the severity of the disease instead of its long-term nature. This suggests health educators needed to revisit the structure of their education programme and the tools used to assess it.
Teaching methods
To optimise the effects of health education, the content must be appropriate for people with COPD (Hyland et al., 2006; White et al., 2006). Further, the method of transmitting the health education programme must suit COPD patients. The COPD-X Plan (Yang et al., 2018) suggested that interactive sessions were more effective than lecturing. It is through interactive discussions on various topics that real meaning and understanding is developed over time.
This type of education session encourages full participation and offers opportunity to engage in the lessons. This also helps participants remember the information, yielding benefits over the long term. Pictures and other visual aids can reinforce the lessons. There were some participants who felt uncomfortable about certain issues being discussed in a group setting, for instance living wills and end-of-life. The consensus was that such issues should be addressed in individually tailored discussions (White et al., 2006).
LIMITATIONS
The primary author is a respiratory clinical nurse specialist involved in providing a health education programme to people with COPD. This could have led to bias in the results, especially where the author may have anticipated certain results, leading to a tendency to influence them. To mitigate against this risk, the work was frequently checked by the second author.
Employing a range of studies, underpinned by diverse methodological perspectives, poses challenges in data analysis and integration of results. The heterogeneous interventions reported in the reviewed articles may have limited the results because of the lack of consistency. Also, the study population of the reviewed literature was not limited to one specific ethnicity, presenting a higher chance of this variation affecting the results. Finally, for the benefits of a health education programme to be significant, the follow-up time used in the published research studies needed to be at least one year post-programme. Unfortunately, in most of the studies discussed here, the follow-up was within six months (White et al., 2006). This led to a failure to demonstrate the long-term efficacy of the educational intervention in PRPs.
RECOMMENDATION FOR FUTURE RESEARCH AND CHANGE OF PRACTICE
Health professionals providing PRPs in any setting must consider evaluating the educational component to establish its significance in the programme. The evaluation of a programme will highlight areas of improvement and those requiring change. Knowing the attributes of the educational intervention in a PRP will help health professionals shape the structure of the intervention. As much as the exercise component in PRPs was highly appreciated in the reviewed literature, more emphasis should be focused on research to investigate the significance of education to complement the benefits of exercise. There is a need for mixed-methods research to help health-care professionals select validated measurement tools to evaluate the educational component.
Early education intervention after diagnosis of COPD has the potential to show the influence of the intervention in the management of symptoms. Therefore, education should be provided to people with COPD upon being diagnosed and during the progression of the disease.
The population of people with COPD in Aotearoa New Zealand includes higher proportions of Māori and Pacific people (Winnard et al., 2015). As noted earlier, Māori have the highest rate of COPD mortality, 190.7 deaths per 100,000 people per year, which is 2.24 (95% CI 2.04-2.41) times higher than the rate of 85.1 for non-Māori, Pacific and Asian (Telfar Barnard & Zhang, 2016). COPD is the fourth leading cause of mortality in New Zealand (Milne & Beasley, 2015). Therefore, the education component of PRP must be culturally safe to meet the needs of people with unique cultural backgrounds. It is also pivotal to translat learning materials into different languages. PRP in New Zealand must prioritise Māori and Pacific populations to provide equitable quality health services.
CONCLUSION
A PRP is a comprehensive non-pharmaceutical intervention which includes a thorough patient assessment and the use of exercises to enhance health outcomes. Most recent studies reviewed support the argument that a PRP is beneficial in improving quality of life on completion of the programme. The educational component of a PRP for people with COPD is not supported by sufficient evidence for it to claim its place in such a programme. Further research is needed to investigate the place of the educational component of PRPs in any setting and to test the measurement tools on people with COPD in New Zealand.
Further research is required to:
- measure whether education does influence health outcomes in COPD patients in New Zealand;
- evaluate the teaching methods currently being used in any PRP settings where cultural diversity is prominent in New Zealand;
- investigate the relevance of the topics being covered in the current education component from the patient’s perspective; and
- explore involvement of cultural leaders/peer groups in the delivery of education.
REFERENCES
Alison, J. A., McKeough, Z. J., Johnston, K., McNamara, R. J., Spencer, L. M., Jenkins, S. C., Hill, C. J., McDonald, V. M., Frith, P., Cafarella, P., Brooke, M., Cameron‐Tucker, H. L., Candy, S., Cecins , N., Chan, A. S. L., Dale, M. T., Dowman, L. M., Granger, C., Halloran, S., Jung, P., Lee, A. L., Leung, R., Matulick, T., Osadnik, C., Roberts, M., Walsh, J., Wootton, S., & Holland, A. E., on behalf of the Lung Foundation Australia and the Thoracic Society of Australia and New Zealand. (2017). Australian and New Zealand pulmonary rehabilitation guidelines. Respirology, 22(4), 800-819.
Blackstock, F. C., Webster, K. E., McDonald, C. F., & Hill, C. J. (2014). Comparable improvements achieved in chronic obstructive pulmonary disease through pulmonary rehabilitation with and without a structured educational intervention: A randomized controlled trial. Respirology, 19(2), 193-202.
Brady, S., Lee, N., Gibbons, K., & Bogossian, F. (2019). Woman-centred care: An integrative review of the empirical literature. International Journal of Nursing Studies, 94, 107-119.
Casey, D., Murphy, K., Cooney, A., Mee, L., & Dowling, M. (2011). Developing a structured education programme for clients with COPD. British Journal of Community Nursing, 16(5), 231-237.
Conn, V. S., Valentine, J. C., Cooper, H. M., & Rantz, M. J. (2003). Grey literature in meta-analyses. Nursing Research, 52(4), 256-261.
Crisafulli, E., Loschi, S., Beneventi, C., De Biase, A., Tazzioli, B., Papetti, A., Lorenzi, C., & Clini, E. M. (2010). Learning impact of education during pulmonary rehabilitation program. An observational short-term cohort study. Monaldi Archives for Chest Disease, 73(2), 64-71.
de Torres, J. P., Pinto-Plata, V., Ingenito, E., Bagley, P., Gray, A., Berger, R., & Celli, B. (2002). Power of outcome measurements to detect clinically significant changes in pulmonary rehabilitation of patients with COPD. Chest, 121(4), 1092-1098.
Global Initiative for Chronic Obstructive Lung Disease. (2018). Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease (2018 report).
Global Initiative for Chronic Obstructive Lung Disease. (2019). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2019 report.
Grove, S. K., & Gray, J. R. (2018). Understanding nursing research e-book: Building an evidence-based practice. Elsevier Health Sciences.
Gudmundsson, G., Gislason, T., Janson, C., Lindberg, E., Hallin, R., Ulrik, C. S., Brøndum, E., Nieminen, M. M., Aine, T., & Bakke, P. (2005). Risk factors for rehospitalisation in COPD: Role of health status, anxiety and depression. European Respiratory Journal, 26(3), 414-419.
Harris, M., Smith, B. J., & Veale, A. (2008). Patient education programs – Can they improve outcomes in COPD? International Journal of Chronic Obstructive Pulmonary Disease, 3(1), 109-112.
Hong, Q. N., Fàbregues, S., Bartlett, G., Boardman, F., Cargo, M., Dagenais, P., Gagnon, M.-P., Griffiths, F., Nicolau, B., O’Cathain, A., Rousseau, M.-C., Vedel, I., & Pluye, P. (2018). The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Education for Information, 34(4), 285-291.
Hopia, H., Latvala, E., & Liimatainen, L. (2016). Reviewing the methodology of an integrative review. Scandinavian Journal of Caring Sciences, 30(4), 662-669.
Houghton, T. (2011). Does positivism really ‘work’ in the social sciences. E-International Relations.
Hyland, M. E., Jones, R. C. M., & Hanney, K. E. (2006). The Lung Information Needs Questionnaire: Development, preliminary validation and findings. Respiratory Medicine, 100(10), 1807-1816.
Jang, J. G., Kim, J. S., Chung, J. H., Shin, K. C., Ahn, J. H., Lee, M. S., Bang, S. H., Park, D. Y., Nam, M. J., Jin, H. J., & Lee, K. H. (2019). Comprehensive effects of organized education for patients with chronic obstructive pulmonary disease. International Journal of Chronic Obstructive Pulmonary Disease, 14, 2603-2609.
Jones, R. C., Wang, X., Harding, S., Bott, J., & Hyland, M. (2008). Educational impact of pulmonary rehabilitation: Lung Information Needs Questionnaire. Respiratory Medicine, 102(10), 1439-1445.
Maples, P., Franks, A., Stevens, A. B., & Wallace, L. S. (2010). Development and validation of a low-literacy Chronic Obstructive Pulmonary Disease knowledge Questionnaire (COPD-Q). Patient Education and Counseling, 81(1), 19-22.
Milne, R., & Beasley, R. (2015). Hospital admissions for chronic obstructive pulmonary disease in New Zealand. New Zealand Medical Journal, 128(1408), 23-35.
Monninkhof, E., van der Valk, V. D. P., Van der Palen, J., Van Herwaarden, C., & Zielhuis, G. (2003). Effects of a comprehensive self-management programme in patients with chronic obstructive pulmonary disease. European Respiratory Journal, 22(5), 815-820.
National Collaborating Centre for Chronic Conditions. (2004). Chronic obstructive pulmonary disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary care. Thorax, 59, 1-232.
Neville, S., Napier, S., Adams, J., Wham, C., & Jackson, D. (2016). An integrative review of the factors related to building age‐friendly rural communities. Journal of Clinical Nursing, 25(17-18), 2402-2412.
Nici, L., Raskin, J., Rochester, C. L., Bourbeau, J. C., Carlin, B. W., Casaburi, R., Celli, B., Cote, C., Crouch, R. H., Diez-Morales, L. F., Donner, C. F., Fahy, B. F., Garvey, C., Goldstein, R., Lane-Reticker, A., Lareau, S. C., Make, B., Maltais, F., McCormick, J., Morgan, M. D. L., Ries, A. L., Troosters, T., & ZuWallack, R. (2009). Pulmonary rehabilitation: What we know and what we need to know. Journal of Cardiopulmonary Rehabilitation and Prevention, 29(3), 141-151.
Omachi, T. A., Sarkar, U., Yelin, E. H., Blanc, P. D., & Katz, P. P. (2013). Lower health literacy is associated with poorer health status and outcomes in chronic obstructive pulmonary disease. Journal of General Internal Medicine, 28(1), 74-81.
O’Neill, B., Cosgrove, D., MacMahon, J., McCrum-Gardner, E., & Bradley, J. M. (2012). Assessing education in pulmonary rehabilitation: The understanding COPD (UCOPD) questionnaire. COPD: Journal of Chronic Obstructive Pulmonary Disease, 9(2), 166-174.
Paneroni, M., Clini, E., Crisafulli, E., Guffanti, E., Fumagalli, A., Bernasconi, A., Cabiaglia, A., Nicolini, A., Brogi, S., Ambrosino, N., Peroni, R., Bianchi, L., & Vitacca, M. (2013). Feasibility and effectiveness of an educational program in Italian COPD patients undergoing rehabilitation. Respiratory Care, 58(2), 327-333.
Peterson, P. N., Shetterly, S. M., Clarke, C. L., Bekelman, D. B., Chan, P. S., Allen, L. A., Matlock, D. D., Magid, D. J., & Masoudi, F. A. (2011). Health literacy and outcomes among patients with heart failure. JAMA, 305(16), 1695-1701.
Sandelowsky, H., Krakau, I., Modin, S., Ställberg, B., & Nager, A. (2019). COPD patients need more information about self-management: A cross-sectional study in Swedish primary care. Scandinavian Journal of Primary Health Care, 37(4), 459-467.
Steinsbekk, A., Rygg, L., Lisulo, M., Rise, M. B., & Fretheim, A. (2012). Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysis. BMC Health Services Research, 12(1), 213.
Strömberg, A. (2005). The crucial role of patient education in heart failure. European Journal of Heart Failure, 7(3), 363-369.
Telfar Barnard, L., & Zhang, J. (2016). The impact of respiratory disease in New Zealand: 2016 update.
Terwee, C. B., Bot, S. D., de Boer, M. R., van der Windt, D. A., Knol, D. L., Dekker, J., Bouter, L. M., & de Vet, H. C. (2007). Quality criteria were proposed for measurement properties of health status questionnaires. Journal of Clinical Epidemiology, 60(1), 34-42.
Vestbo, J., Hurd, S. S., Agustí, A. G., Jones, P. W., Vogelmeier, C., Anzueto, A., Barnes, P. J., Fabbri, L. M., Martinez, F. J., Nishimura, M., Stockley, R. A., Sin, D. D., & Rodriguez-Roisi, R. (2013). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. American Journal of Respiratory and Critical Care Medicine, 187(4), 347-365.
White, R., Walker, P., Roberts, S., Kalisky, S., & White, P. (2006). Bristol COPD Knowledge Questionnaire (BCKQ): Testing what we teach patients about COPD. Chronic Respiratory Disease, 3(3), 123-131.
Whittemore, R., & Knafl, K. (2005). The integrative review: Updated methodology. Journal of Advanced Nursing, 52(5), 546-553.
Wilson, J. S., O’Neill, B., Reilly, J., MacMahon, J., & Bradley, J. M. (2007). Education in pulmonary rehabilitation: The patient’s perspective. Archives of Physical Medicine and Rehabilitation, 88(12), 1704-1709.
Winnard, D., Lee, M., & Macleod, G. (2015). Demographic profile: 2013 census, population of Counties Manukau. Counties Manukau Health.
Wright‐St Clair, V. A., Neville, S., Forsyth, V., White, L., & Napier, S. (2017). Integrative review of older adult loneliness and social isolation in Aotearoa/New Zealand. Australasian Journal on Ageing, 36(2), 114-123.
Yang, I. A., Brown, J. L., George, J., Jenkins, S., McDonald, C. F., McDonald, V., Smith, B., Zwar, N., & Dabscheck, E. (2018). The COPD-X plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease 2018 [Version 2.56].
Zeng, Y., Jiang, F., Chen, Y., Chen, P., & Cai, S. (2018). Exercise assessments and trainings of pulmonary rehabilitation in COPD: A literature review. International Journal of Chronic Obstructive Pulmonary Disease, 13, 2013-2023.
Daily doses – uncut news
| 22 Jul |
Te Whatu Ora must disclose staffing levels at time of tragic deathTe Whatu Ora must disclose whether the Waikato emergency department (ED) was short-staffed at the time a man tragically died in the waiting room, NZNO says. |
| 6 Jul |
Reflecting on IND 2026Looking back on last month’s International Nurses Day 12 May 2026 (IND 2026), the impact of this year's theme "Our Nurses. Our Future. Empowered Nurses Save Lives" continues to resonate across the world. ICN’s landmark IND 2026 report defined seven key powers of nursing and this message has been strengthened with nurses in every region celebrating, naming, and owning their powers throughout May. |
| 3 Jul |
Health New Zealand acknowledges Ombudsman statement on Wakari Ward 10AHealth NZ welcomes the independent investigation by the Ministry of Health into Ward 10A. On Wednesday the Health NZ board agreed to close Wakari Ward 10a as a forensic intellectual disability (ID) unit, with the future use of the ward yet to be determined. |
| 2 Jul |
New programme to fast track bowel cancer care and cut colonoscopy waitlistsHealth New Zealand is today launching a national initiative, designed to fast track bowel cancer care and reduce colonoscopy waitlists by up to 30 per cent. |
| 1 Jul |
Six new Co-Response Team locations announced to strengthen support for people in mental distressThe next six locations for Health New Zealand and NZ Police Co-Response Teams have been confirmed, expanding a model that helps people experiencing mental distress receive timely, wraparound support that better meets their health needs. |
| 29 Jun |
Mental health and addiction targets progress continuesHealth New Zealand continues to make important progress against its mental health and addiction targets, meeting four out of five national targets this quarter. |
| 25 Jun |
Access to care continuing to improve across a range of health indicatorsNew health data released today shows continued improvement in access to care across a range of health indicators. |
| 18 Jun |
Funding "boost" continues dangerous under-funding of aged careThe Health Minister’s funding "boost" for aged residential care continues underfunding to the sector and will continue unsafe practices and short staffing, which is putting vulnerable residents at risk, NZNO says. |
| 16 Jun |
Labour to make maternity scans freeLabour will add free maternity scans to the Medicard alongside three free doctor’s visits a year, so every pregnant woman gets the care she needs. |
| 29 May |
WellSouth Statement on Budget 2026: a missed opportunityBudget 2026 is a missed opportunity for primary care, and for the communities that depend on it most, in particular our rural people and practices. |
| 29 May |
Updated - Nurses on front lines of Ebola outbreak at serious riskIn response to the gravely concerning and escalating Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda, the International Council of Nurses (ICN) warns that nurses and other frontline health workers are being put at serious risk and left fearful for their safety. |
| 27 May |
Health NZ committed to safeguarding patient informationHealth New Zealand welcomes the reports released today into the Manage My Health (MMH) cyber incident and is committed to ensuring all possible steps are taken to safeguard patient information. |
| 22 May |
More New Zealanders could benefit from funded vaccines from 2027Pharmac is proposing changes that would give more New Zealanders access to funded vaccines from 2027, including expanded access to the flu vaccine for young children. |
| 21 May |
It’s not just the wallet: How the gender pay gap can hurt women’s bodiesWhile many aspects of New Zealand’s enduring gender pay gap have been discussed, its physical impact on workers has been largely overlooked – until now. |
| 21 May |
Bupa nurses take pay equity claim over historic wage discriminationNZNO nurses working at Bupa aged residential care homes throughout Aotearoa New Zealand have raised a pay equity claim to address historic gender-based wage discrimination. |
| 20 May |
Waikato Hospital adds 10 forensic mental health beds Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
Ten new forensic inpatient beds have been made available at the Regional Forensic Psychiatric Service at Waikato Hospital to expand forensic mental health capacity for adults in prison or on remand in Health New Zealand’s Midland region.
|
| 18 May |
Strong gains in two-year immunisation target for Tamariki MāoriHealth New Zealand is welcoming a significant increase in Māori immunisation rates, with full immunisation at 24 months rising from just over 60 per cent in late 2024 to 71.5 per cent at the end of last month. |
| 15 May |
New global report shows empowering nurses is key to saving lives and strengthening health systemsAs the world marks International Nurses Day, the International Council of Nurses (ICN) is calling for urgent investment in nursing, supported by a major new global report, Our Nurses. Our Future. Empowered Nurses Save Lives, that presents seven key nursing powers. |
| 14 May |
Lakes and Whanganui nurses still waiting for Holiday Pay a decade on
Photo by Fin Ocheduszko-Brown at Whanganui Chronicle Nurses at Lakes and Whanganui districts are calling on Te Whatu Ora to explain why after a decade of redress, they still don’t know when they will receive their full Holiday Act remediation payments, NZNO says. |
| 13 May |
Recognising the extraordinary contribution of nursesInternational Nurses Day is an opportunity to recognise the extraordinary role nurses play in caring for New Zealanders at every stage of life, Health Minister Simeon Brown says. |
| 12 May |
Government’s decision to scrap fees free scheme will lead to further student exodusThe Coalition Government’s decision to scrap the fees free policy for third year tertiary students has left nursing tauira outraged |
| 30 Apr |
BroPilot grounding digital tools in whānau, culture, and care A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
A passion for his Māori culture and a desire to make AI accessible to everyone inspired Troy Baker, Senior ICT Specialist, Health New Zealand to develop BroPilot – a culturally grounded way of working with Microsoft Copilot that reflects Māori values, whakaaro, and real lived experience.
|
| 29 Apr |
Heartbreaking tragedies were avoidable - NZNOAnalysis by a media outlet, published today, finding health care staff shortages were contributing factors in the deaths of 11 babies is a national and avoidable tragedy, NZNO says. |
| 28 Apr |
CTU launches Roving Health and Safety Representatives policy on Workers’ Memorial DayThe New Zealand Council of Trade Unions Te Kauae Kaimahi has today launched our Roving Health and Safety Representatives policy at the Workers’ Memorial Day commemoration in Wellington, with further events held across the motu in Manawatū, Christchurch, and Otago. |
| 24 Apr |
“The 80s Calling”: New national campaign challenges outdated HIV stigmaAssociate Health Minister Matt Doocey today launched Health New Zealand’s “The 80s Calling”; a provocative new campaign designed to reduce stigma, normalise conversations about HIV, and support people living with HIV. |
| 23 Apr |
Government’s attack on Māori health raised at the UNConcerns over the Coalition Government’s active reversal of policies designed to improve Māori health outcomes were raised at the United Nations in New York this morning. |
| 16 Apr |
Tribute to Professor Lester Levy’s service to healthcareHealth New Zealand Chief Executive Dr Dale Bramley is paying tribute to Health NZ Board Chair Professor Lester Levy, who finishes in the role at the end of the month. |
| 10 Apr |
Chronic health care assistant short staffing harming vulnerable patientsTe Whatu Ora’s attempt to cut costs by requiring health care assistants to carry out cohort patient watches is harming vulnerable patients and staff, NZNO says. |
| 9 Apr |
New group education clinics speeding up knee and hip surgery careHealth New Zealand is rolling out a new group education approach for people waiting for hip and knee surgery in north and west Auckland, resulting in more patients being seen sooner. |
| 25 Mar |
National Diabetes Roadmap launched to improve care, prevention, and quality of lifeHealth New Zealand has launched a new National Diabetes Roadmap (‘the Roadmap’) to improve care, strengthen prevention, and support better health outcomes and quality of life for people living with diabetes. |
| 24 Mar |
ACT should leave nursing to professionals and medical evidenceTōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO Kaiwhakahaere Kerri Nuku says ACT MP Todd Stephenson has dismissed the Nursing Council’s draft code of conduct - which proposes strengthening cultural safety, whānau-centred care and te Tiriti o Waitangi obligations - as political ideology. |
| 23 Mar |
UK report reflects ICN warnings on international recruitment ripoff — now countries must act togetherThe International Council of Nurses (ICN) warmly welcomes a new report from the UK All Party Parliamentary Group (APPG) on Global Health and Security that recognizes the huge sums saved by high-income countries who recruit abroad and acknowledges the severe harms caused by unethical recruitment from fragile source countries left without nurses. |
| 20 Mar |
HPV self-test boosts cervical cancer screening ‘across the board’, new study confirmsMaking human papillomavirus (HPV) self-testing available to all women increases the number of people screened for cervical cancer, a new study led by researchers from Te Herenga Waka—Victoria University of Wellington has confirmed. |
| 19 Mar |
ICN at CSW70: Violence against nurses is a gendered crisis threatening global healthThe International Council of Nurses (ICN) has warned that violence against nurses is a global gendered crisis that threatens health systems, patient safety and workforce sustainability |
| 17 Mar |
Additional winter health care workers a drop in the ocean of needThe Government’s announcement today of 378 extra staff to help hospitals cope with winter demand is a drop in the ocean of what patients need, NZNO says. |
| 12 Mar |
Funding change will ensure more consistent emergency care for New ZealandersA simple change in how ambulance medicines are funded is set to create more consistent emergency care. |
| 9 Mar |
Questions over dilapidated and cramped renal unit forced to ration dialysisThe Health Minister must explain why after years of concerns from nurses about Christchurch Hospital’s barely functioning dialysis unit, he only stepped in late yesterday when life-saving treatment had to be rationed, NZNO says. |
| 3 Mar |
Hospitals and health workers should never be targetsThe right of health care workers to provide care during international conflicts must be protected, Tōpūtanga Tapuhi Kaitiaki o Aotearoa NZNO says. |
| 2 Mar |
Public and Mental Health Nurses settle collective agreementHealth New Zealand welcomes the ratification of the two Public Service Association (PSA) Public and Mental Health Nurses collective employment agreements for Auckland and the Rest of New Zealand. |


